

Expected impact of MRI-related interreader variability on ProScreen prostate cancer screening trial: a pre-trial validation study
- PMID: 33036660
- PMCID: PMC7547469
- DOI: 10.1186/s40644-020-00351-w
Expected impact of MRI-related interreader variability on ProScreen prostate cancer screening trial: a pre-trial validation study
Abstract
Background: The aim of this study is to investigate the potential impact of prostate magnetic resonance imaging (MRI) -related interreader variability on a population-based randomized prostate cancer screening trial (ProScreen).
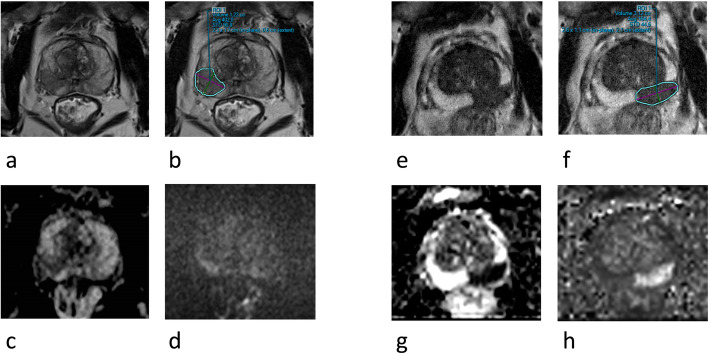
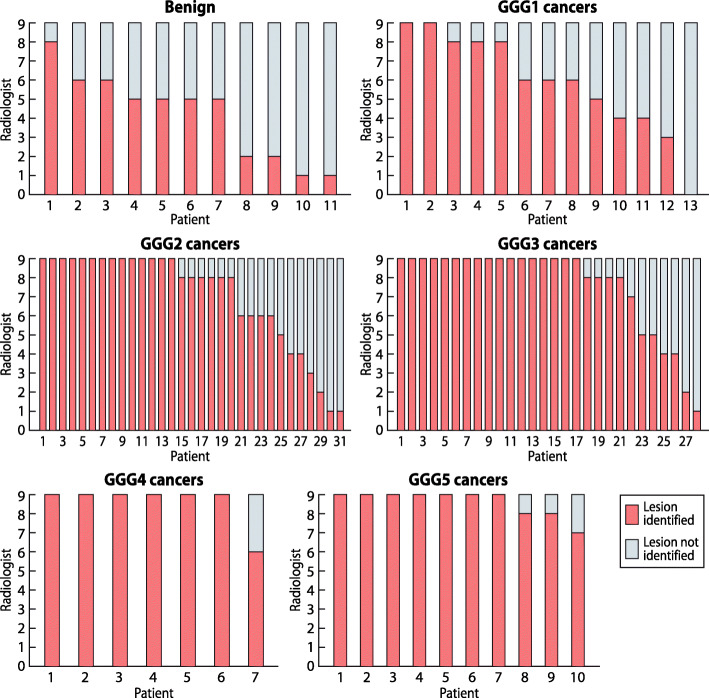
Methods: From January 2014 to January 2018, 100 men aged 50-63 years with clinical suspicion of prostate cancer (PCa) in Helsinki University Hospital underwent MRI. Nine radiologists individually reviewed the pseudonymized MRI scans of all 100 men in two ProScreen trial centers. All 100 men were biopsied according to a histological composite variable comprising radical prostatectomy histology (N = 38) or biopsy result within 1 year from the imaging (N = 62). Fleiss' kappa (κ) was used to estimate the combined agreement between all individual radiologists. Sample data were subsequently extrapolated to 1000-men subgroups of the ProScreen cohort.
Results: Altogether 89% men of the 100-men sample were diagnosed with PCa within a median of 2.4 years of follow-up. Clinically significant PCa (csPCa) was identified in 76% men. For all PCa, mean sensitivity was 79% (SD ±10%, range 62-96%), and mean specificity 60% (SD ±22%, range 27-82%). For csPCa (Gleason Grade 2-5) MRI was equally sensitive (mean 82%, SD ±9%, range 67-97%) but less specific (mean 47%, SD ±20%, range 21-75%). Interreader agreement for any lesion was fair (κ 0.40) and for PI-RADS 4-5 lesions it was moderate (κ 0.60). Upon extrapolating these data, the average sensitivity and specificity to a screening positive subgroup of 1000 men from ProScreen with a 30% prevalence of csPCa, 639 would be biopsied. Of these, 244 men would be true positive, and 395 false positive. Moreover, 361 men would not be referred to biopsy and among these, 56 csPCas would be missed. The variation among the radiologists was broad as the least sensitive radiologist would have twice as many men biopsied and almost three times more men would undergo unnecessary biopsies. Although the most sensitive radiologist would miss only 2.6% of csPCa (false negatives), the least sensitive radiologist would miss every third.
Conclusions: Interreader agreement was fair to moderate. The role of MRI in the ongoing ProScreen trial is crucial and has a substantial impact on the screening process.
Keywords: Agreement; Magnetic resonance imaging; PI-RADS version 2; Prostate cancer; Screening.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Drost FH, Osses DF, Nieboer D, Steyerberg EW, Bangma CH, Roobol MJ, et al. Prostate magnetic resonance imaging, with or without magnetic resonance imaging-targeted biopsy, and systematic biopsy for detecting prostate cancer: a cochrane systematic review and meta-analysis. Eur Urol. 2020;77:78–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
