

Trends in urologic oncology clinical practice and medical education under COVID-19 pandemic: An international survey of senior clinical and academic urologists
- PMID: 33036903
- PMCID: PMC7539173
- DOI: 10.1016/j.urolonc.2020.09.015
Trends in urologic oncology clinical practice and medical education under COVID-19 pandemic: An international survey of senior clinical and academic urologists
Abstract
Objective: Ad-hoc guidelines for managing the COVID-19 pandemic are published worldwide. We investigated international applications of such policies in the urologic-oncology community.
Methods: A 20-item survey was e-mailed via SurveyMonkey to 100 international senior urologic-oncology surgeons. Leaders' policies regarding clinical/surgical management and medical education were surveyed probing demographics, affiliations, urologic-oncologic areas of interest, and current transportation restrictions. Data on COVID-19 burden were retrieved from the ECDC. Statistical analyses employed non-parametric tests (SPSS v.25.0, IBM).
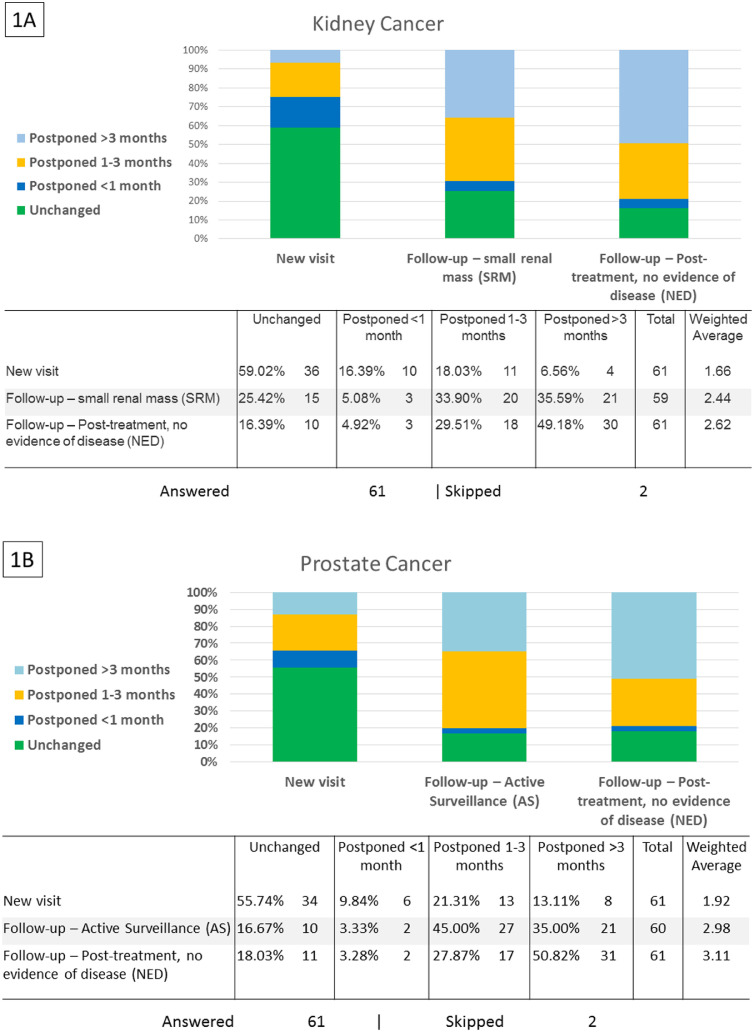
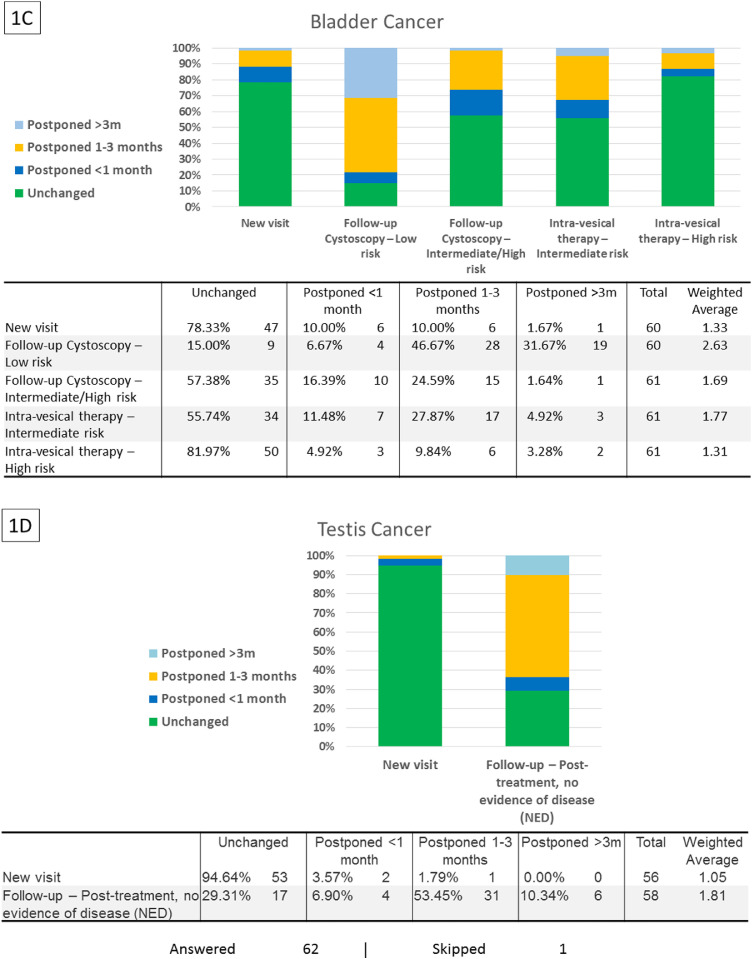
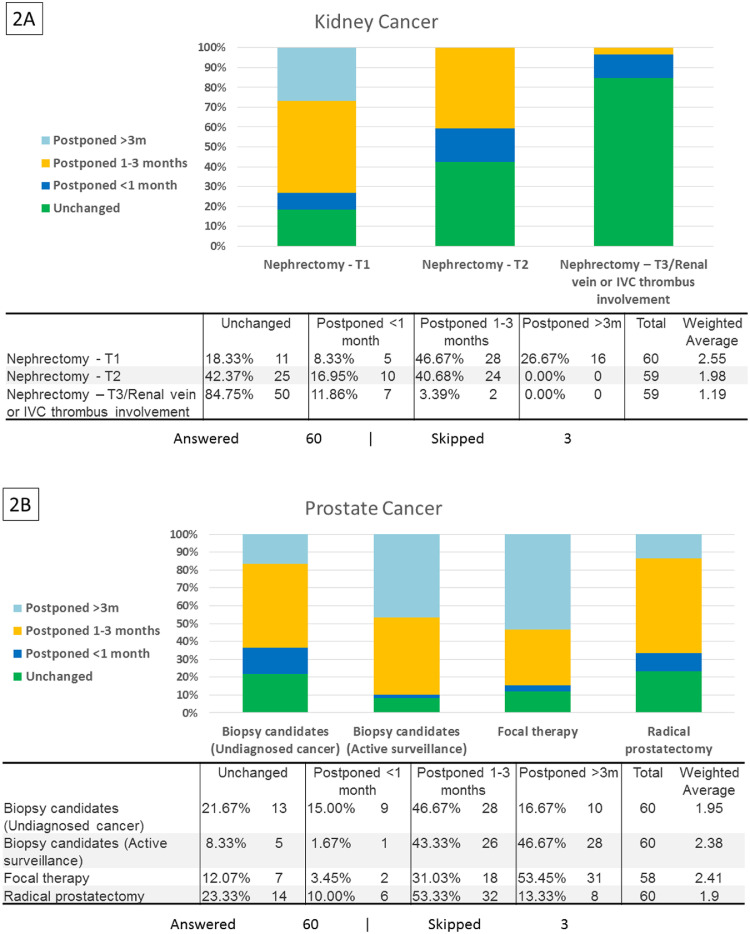
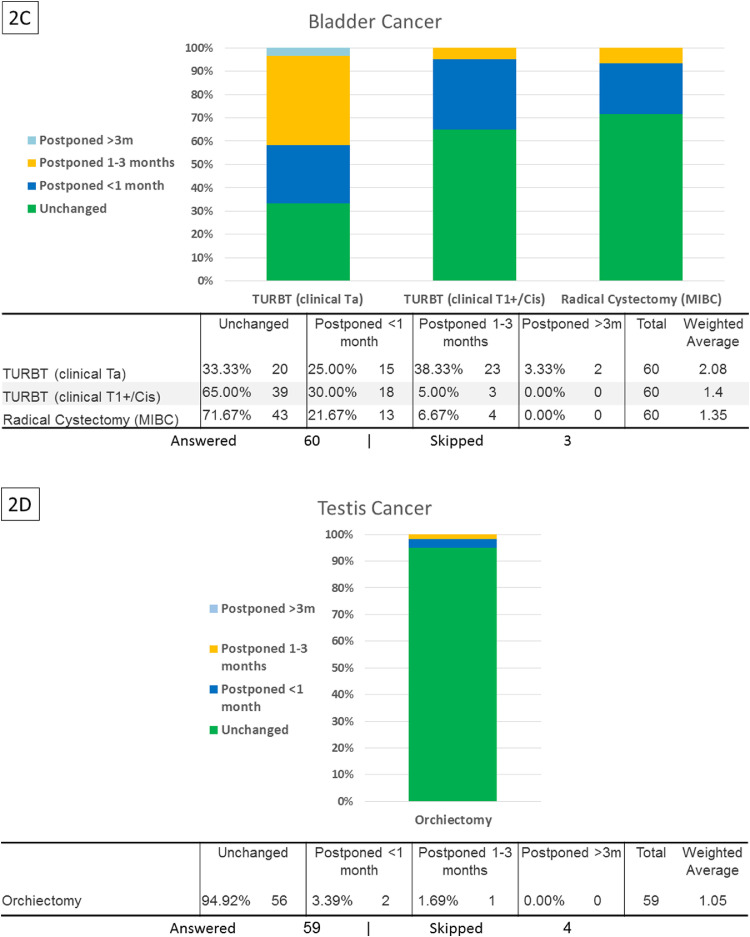
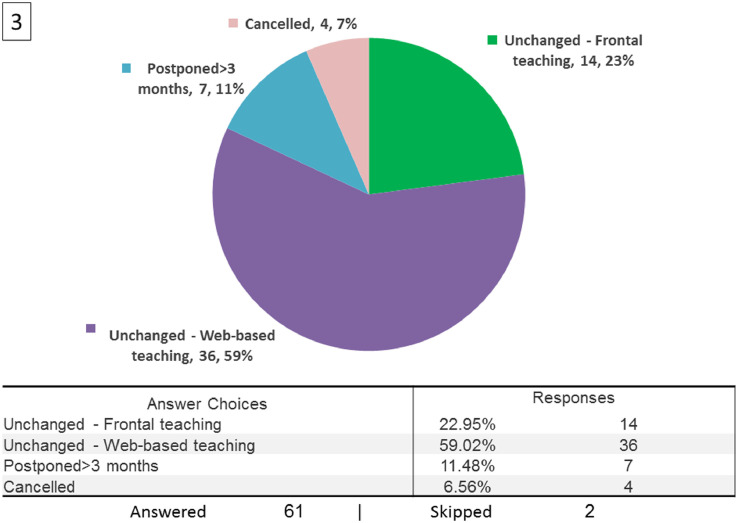
Results: Of 100 leaders from 17 countries, 63 responded to our survey, with 58 (92%) reporting university and/or cancer-center affiliations. Policies on new-patient visits remained mostly unchanged, while follow-up visits for low-risk diseases were mostly postponed, for example, 83.3% for small renal mass (SRM). Radical prostatectomy was delayed in 76.2% of cases, while maintaining scheduled timing for radical cystectomy (71.7%). Delays were longer in Europe than in the Americas for kidney cancer (SRM follow-up, P = 0.014), prostate cancer (new visits, P = 0.003), and intravesical therapy for intermediate-risk bladder cancer (P = 0.043). In Europe, COVID-19 burden correlated with policy adaptation, for example, nephrectomy delays for T2 disease (r = 0.5, P =0.005). Regarding education policies, trainees' medical education was mainly unchanged, whereas senior urologists' planned attendance at professional meetings dropped from 6 (IQR 1-11) to 2 (IQR 0-5) (P < 0.0001).
Conclusion: Under COVID-19, senior urologic-oncology surgeons worldwide apply risk-stratified approaches to timing of clinical and surgical schedules. Policies regarding trainee education were not significantly affected. We suggest establishment of an international consortium to create a directive for coping with such future challenges to global healthcare.
Keywords: Bladder cancer; COVID-19 pandemic; Kidney cancer; Medical education; Policy; Prostate cancer; Testicular cancer; Urologic oncology.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Forecasting the Future of Urology Practice: A Comprehensive Review of the Recommendations by International and European Associations on Priority Procedures During the COVID-19 Pandemic.Eur Urol Focus. 2020 Sep 15;6(5):1032-1048. doi: 10.1016/j.euf.2020.05.007. Epub 2020 May 31. Eur Urol Focus. 2020. PMID: 32553544 Free PMC article. Review.
-
Global change of surgical and oncological clinical practice in urology during early COVID-19 pandemic.World J Urol. 2021 Sep;39(9):3139-3145. doi: 10.1007/s00345-020-03333-6. Epub 2020 Jul 4. World J Urol. 2021. PMID: 32623500 Free PMC article.
-
Urologic oncology case volume among early career urologists: An analysis of certification data from the American board of urology between 2003 and 2019.Urol Oncol. 2025 May;43(5):335.e9-335.e15. doi: 10.1016/j.urolonc.2024.09.034. Epub 2024 Oct 10. Urol Oncol. 2025. PMID: 39393994
-
A Systematic Review on Guidelines and Recommendations for Urology Standard of Care During the COVID-19 Pandemic.Eur Urol Focus. 2020 Sep 15;6(5):1070-1085. doi: 10.1016/j.euf.2020.05.020. Epub 2020 Jun 5. Eur Urol Focus. 2020. PMID: 32532703 Free PMC article.
-
Developments in urologic oncology 'OncoForum': The best of 2014.Actas Urol Esp. 2015 Jun;39(5):271-8. doi: 10.1016/j.acuro.2015.02.004. Epub 2015 Mar 12. Actas Urol Esp. 2015. PMID: 25770399 English, Spanish.
Cited by
-
Education and Training Adaptations for Health Workers during the COVID-19 Pandemic: A Scoping Review of Lessons Learned and Innovations.Healthcare (Basel). 2023 Nov 4;11(21):2902. doi: 10.3390/healthcare11212902. Healthcare (Basel). 2023. PMID: 37958046 Free PMC article.
-
Association between COVID-19 Burden, Population Vaccination Status, and Urologic Oncology Surgery Volume: A National Multicenter Cross-Sectional Study.J Clin Med. 2022 Nov 29;11(23):7071. doi: 10.3390/jcm11237071. J Clin Med. 2022. PMID: 36498646 Free PMC article.
-
Patient Preferences for Treatment of Bacillus Calmette-Guérin-unresponsive Non-muscle-invasive Bladder Cancer: A Cross-country Choice Experiment.Eur Urol Open Sci. 2023 Jan 31;49:92-99. doi: 10.1016/j.euros.2022.12.016. eCollection 2023 Mar. Eur Urol Open Sci. 2023. PMID: 36874596 Free PMC article.
-
The Impact of the COVID-19 Pandemic on Bladder Cancer Care in the Netherlands.Bladder Cancer. 2022 Jun 3;8(2):139-154. doi: 10.3233/BLC-211608. eCollection 2022. Bladder Cancer. 2022. PMID: 38993368 Free PMC article.
-
Impact of the COVID-19 Pandemic on Urologic Oncology Surgery: Implications for Moving Forward.J Clin Med. 2021 Dec 29;11(1):171. doi: 10.3390/jcm11010171. J Clin Med. 2021. PMID: 35011911 Free PMC article.
References
-
- Coronavirus disease 2019 n.d. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed April 12, 2020).
-
- Maria J. Ribal, Philip Cornford, Alberto Briganti, Thomas Knoll, Stavros Gravas, Marek, et al. EAU Guidelines Office Rapid Reaction Group: an organisation-wide collaborative effort to adapt the EAU guidelines recommendations to the COVID-19 era. n.d.https://uroweb.org/wp-content/uploads/EAU-Guidelines-Office-Rapid-Reacti... (accessed April 25, 2020). - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
