

Virological outcome among HIV infected patients transferred from pediatric care to adult units in Madrid, Spain (1997-2017)
- PMID: 33037235
- PMCID: PMC7547007
- DOI: 10.1038/s41598-020-70861-x
Virological outcome among HIV infected patients transferred from pediatric care to adult units in Madrid, Spain (1997-2017)
Abstract
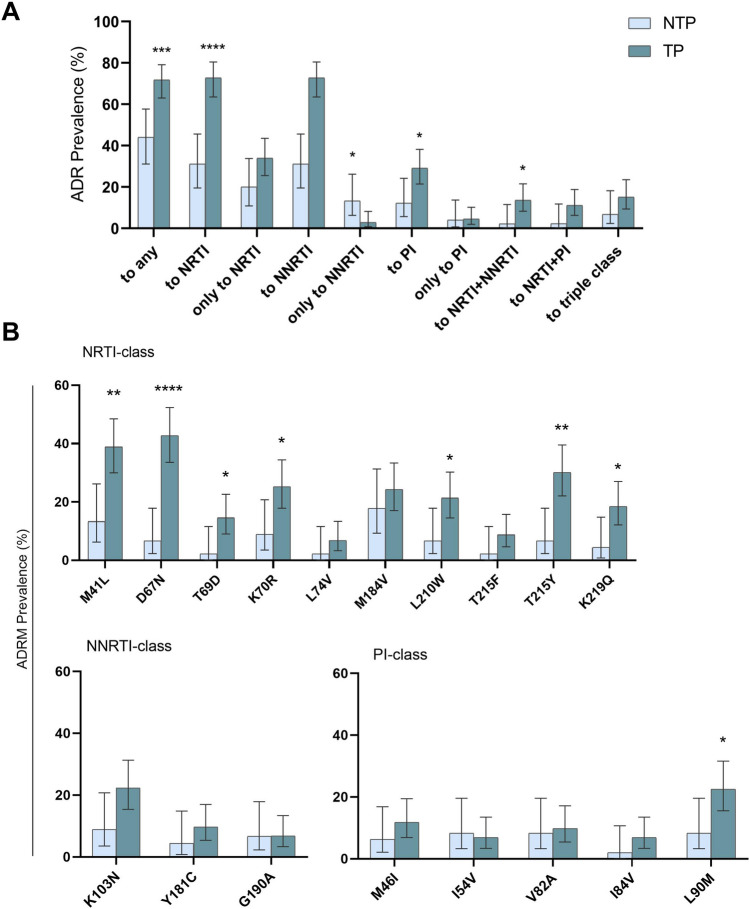
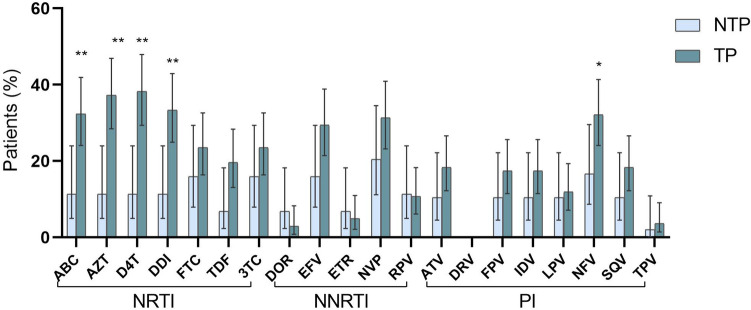
The aim of this transversal study was to describe the virological and immunological features of HIV-infected youths transferred from pediatric to adult care units since 1997 vs. the non-transferred patients from the Madrid Cohort of HIV-infected children and adolescents in Spain. We included 106 non-transferred and 184 transferred patients under clinical follow-up in 17 public hospitals in Madrid by the end of December 2017. Virological and immunological outcomes were compared in transferred vs. non-transferred patients. ART drug resistance mutations and HIV-variants were analyzed in all subjects with available resistance pol genotypes and/or genotypic resistance profiles. Among the study cohort, 133 (72.3%) of 184 transferred and 75 (70.7%) of 106 non-transferred patients had available resistance genotypes. Most (88.9%) of transferred had ART experience at sampling. A third (33.3%) had had a triple-class experience. Acquired drug resistance (ADR) prevalence was significantly higher in pretreated transferred than non-transferred patients (71.8% vs. 44%; p = 0.0009), mainly to NRTI (72.8% vs. 31.1%; p < 0.0001) and PI (29.1% vs. 12%; p = 0.0262). HIV-1 non-B variants were less frequent in transferred vs. non-transferred (6.9% vs. 32%; p < 0.0001). In conclusion, the frequent resistant genotypes found in transferred youths justifies the reinforcement of HIV resistance monitoring after the transition to avoid future therapeutic failures.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- UNAIDS data 2019|UNAIDS. https://www.unaids.org/en/resources/documents/2019/2019-UNAIDS-data.
-
- HIV and AIDS in Adolescents—UNICEF Data. https://data.unicef.org/topic/adolescents/hiv-aids/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
