

Personalized Cancer Vaccines: Clinical Landscape, Challenges, and Opportunities
- PMID: 33038322
- PMCID: PMC7854282
- DOI: 10.1016/j.ymthe.2020.09.038
Personalized Cancer Vaccines: Clinical Landscape, Challenges, and Opportunities
Abstract
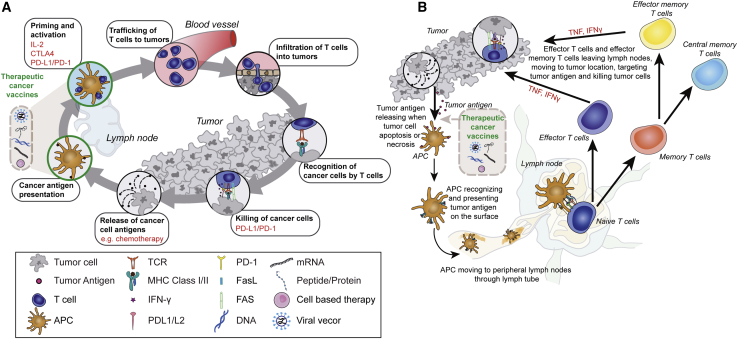
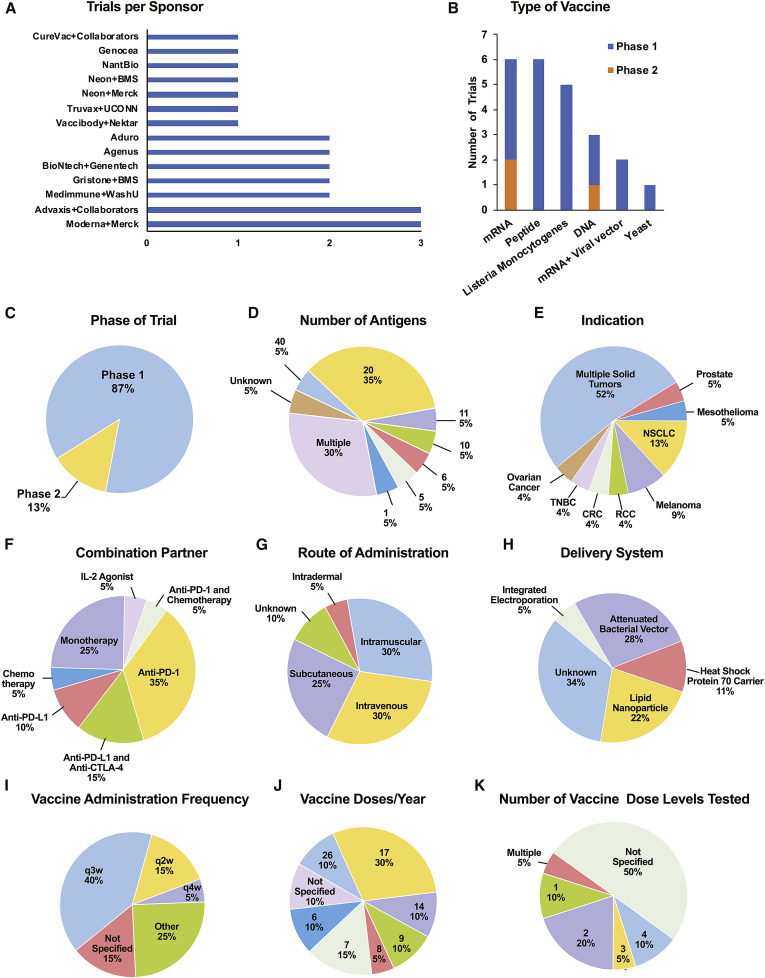
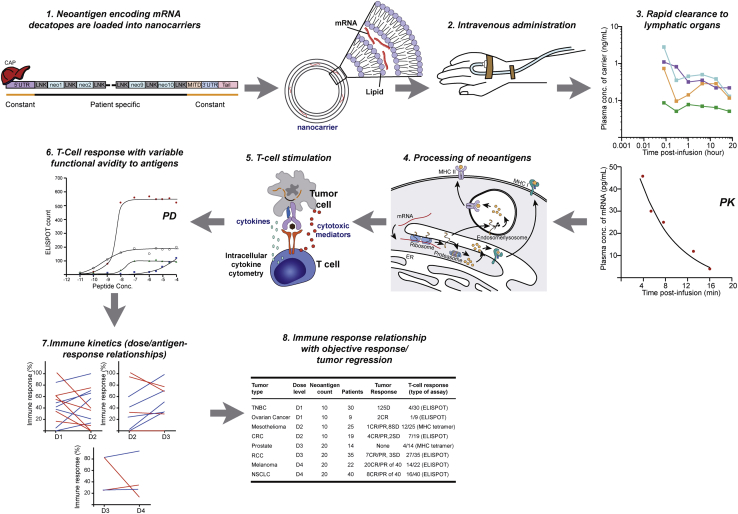
Tremendous innovation is underway among a rapidly expanding repertoire of promising personalized immune-based treatments. Therapeutic cancer vaccines (TCVs) are attractive systemic immunotherapies that activate and expand antigen-specific CD8+ and CD4+ T cells to enhance anti-tumor immunity. Our review highlights key issues impacting TCVs in clinical practice and reports on progress in development. We review the mechanism of action, immune-monitoring, dosing strategies, combinations, obstacles, and regulation of cancer vaccines. Most trials of personalized TCVs are ongoing and represent diverse platforms with predominantly early investigations of mRNA, DNA, or peptide-based targeting strategies against neoantigens in solid tumors, with many in combination immunotherapies. Multiple delivery systems, routes of administration, and dosing strategies are used. Intravenous or intramuscular administration is common, including delivery by lipid nanoparticles. Absorption and biodistribution impact antigen uptake, expression, and presentation, affecting the strength, speed, and duration of immune response. The emerging trials illustrate the complexity of developing this class of innovative immunotherapies. Methodical testing of the multiple potential factors influencing immune responses, as well as refined quantitative methodologies to facilitate optimal dosing strategies, could help resolve uncertainty of therapeutic approaches. To increase the likelihood of success in bringing these medicines to patients, several unique development challenges must be overcome.
Keywords: adjuvant; cancer immunotherapy; clinical pharmacology; clinical trials; drug development; personalized therapeutic cancer vaccine; tumor neoantigen.
Copyright © 2020 The American Society of Gene and Cell Therapy. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Finn O.J. The dawn of vaccines for cancer prevention. Nat. Rev. Immunol. 2018;18:183–194. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
