

Key Parameters of Tumor Epitope Immunogenicity Revealed Through a Consortium Approach Improve Neoantigen Prediction
- PMID: 33038342
- PMCID: PMC7652061
- DOI: 10.1016/j.cell.2020.09.015
Key Parameters of Tumor Epitope Immunogenicity Revealed Through a Consortium Approach Improve Neoantigen Prediction
Abstract
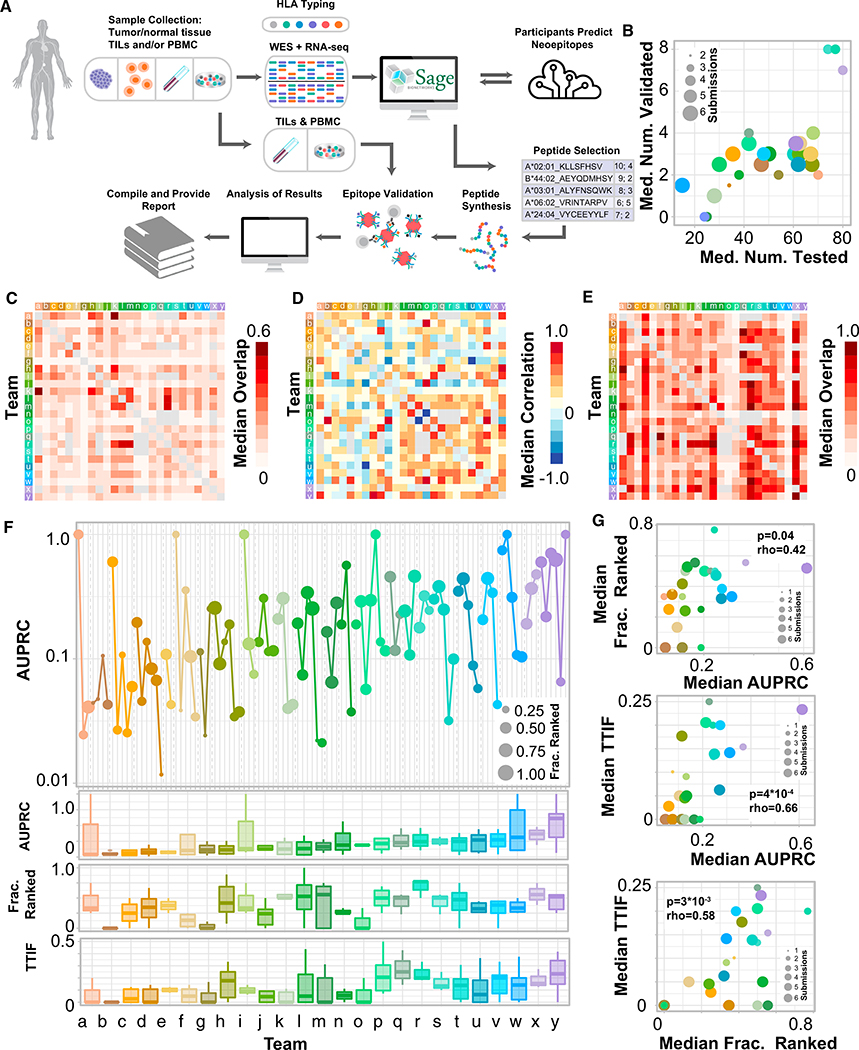
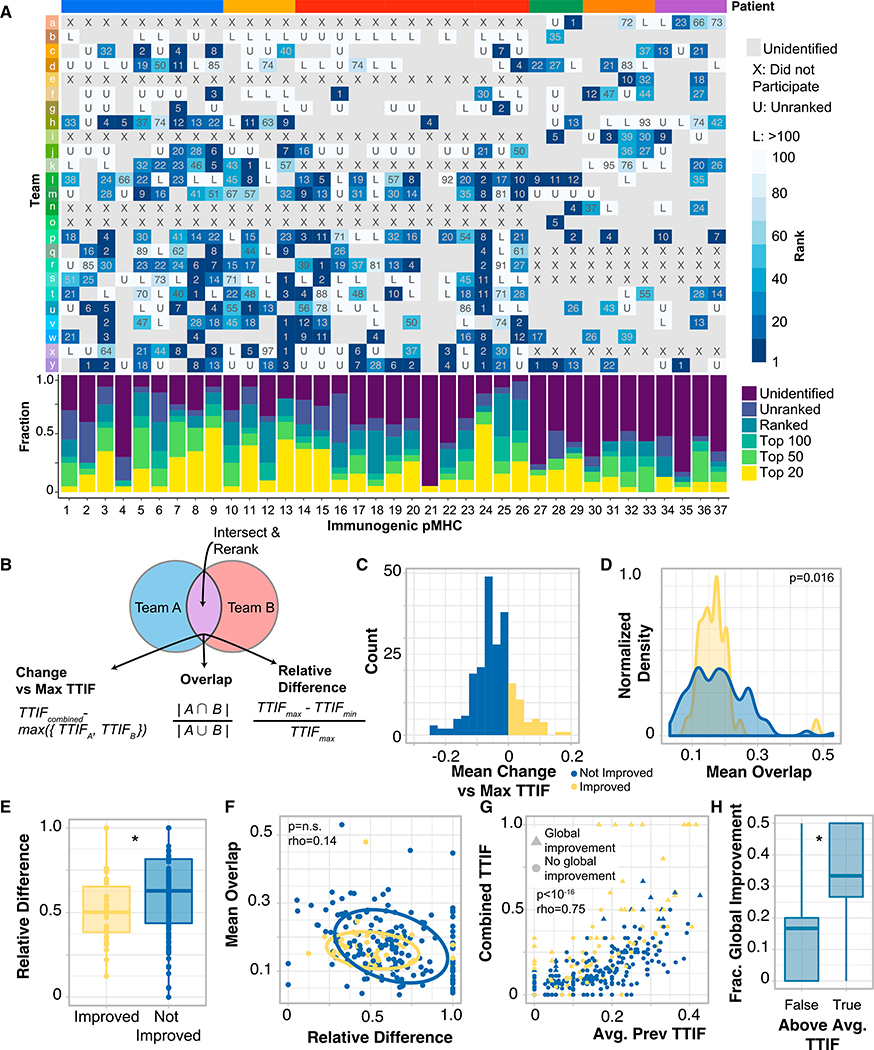
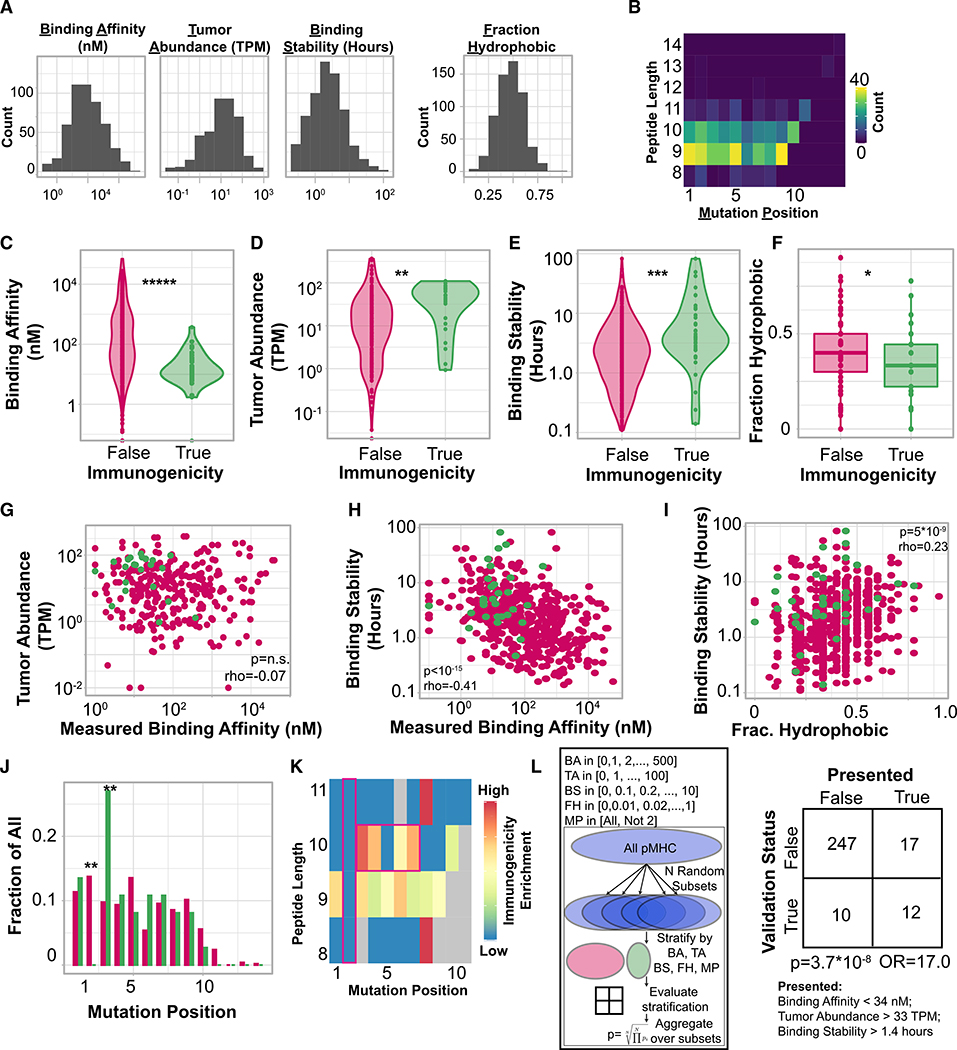
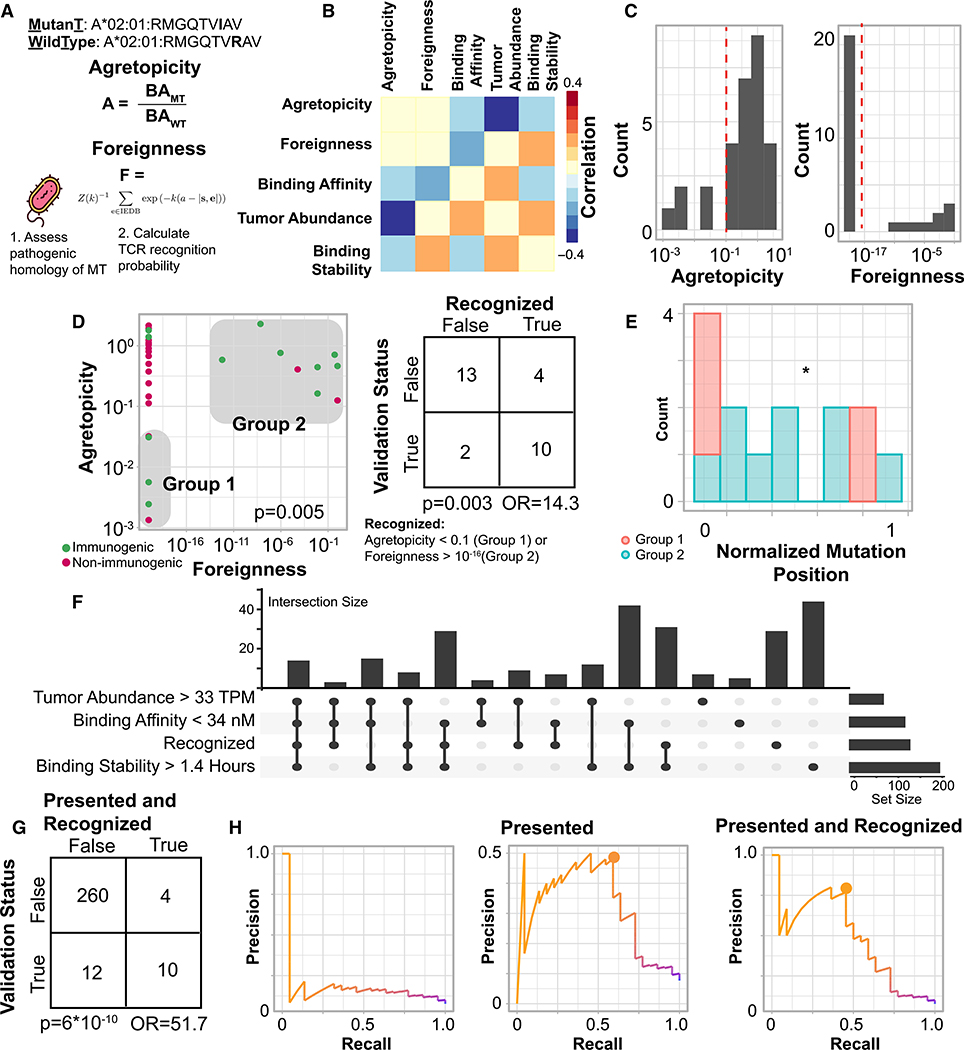
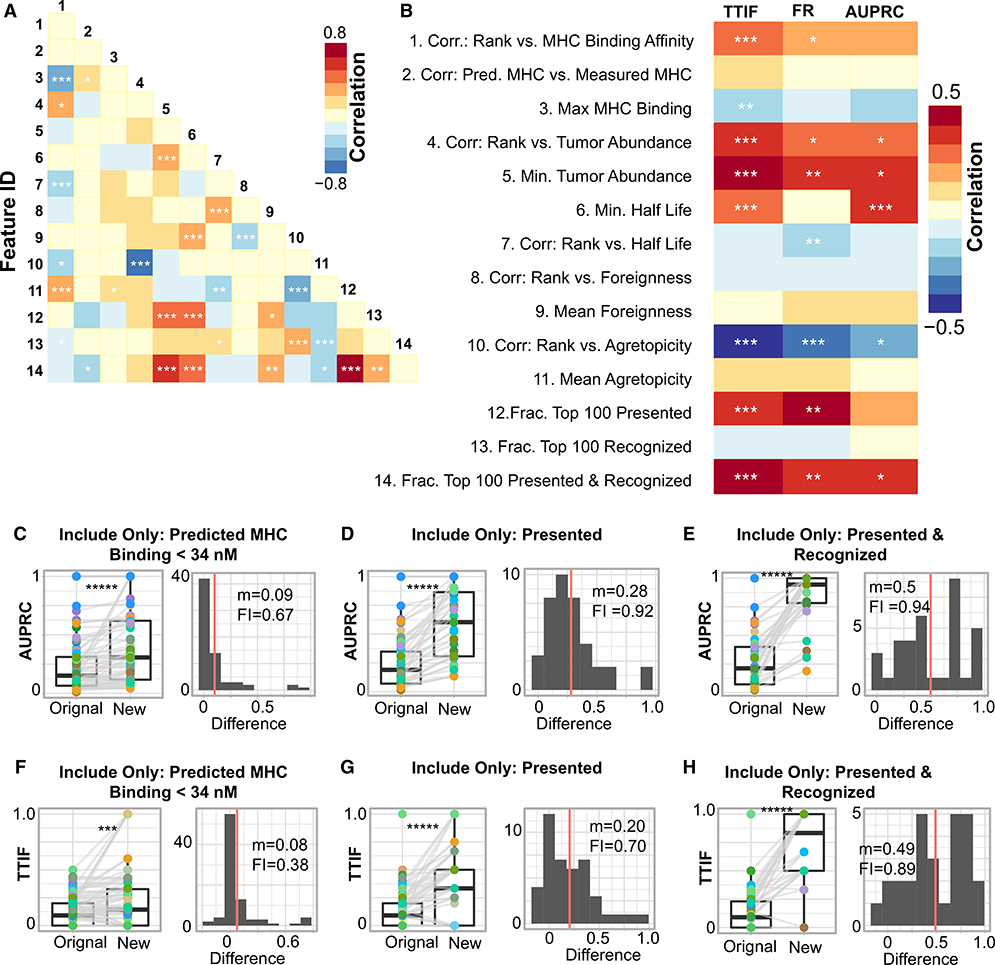
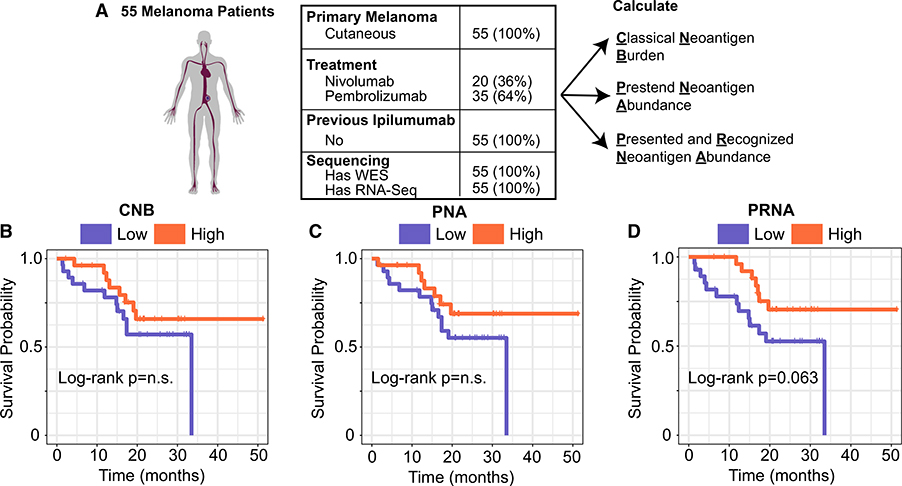
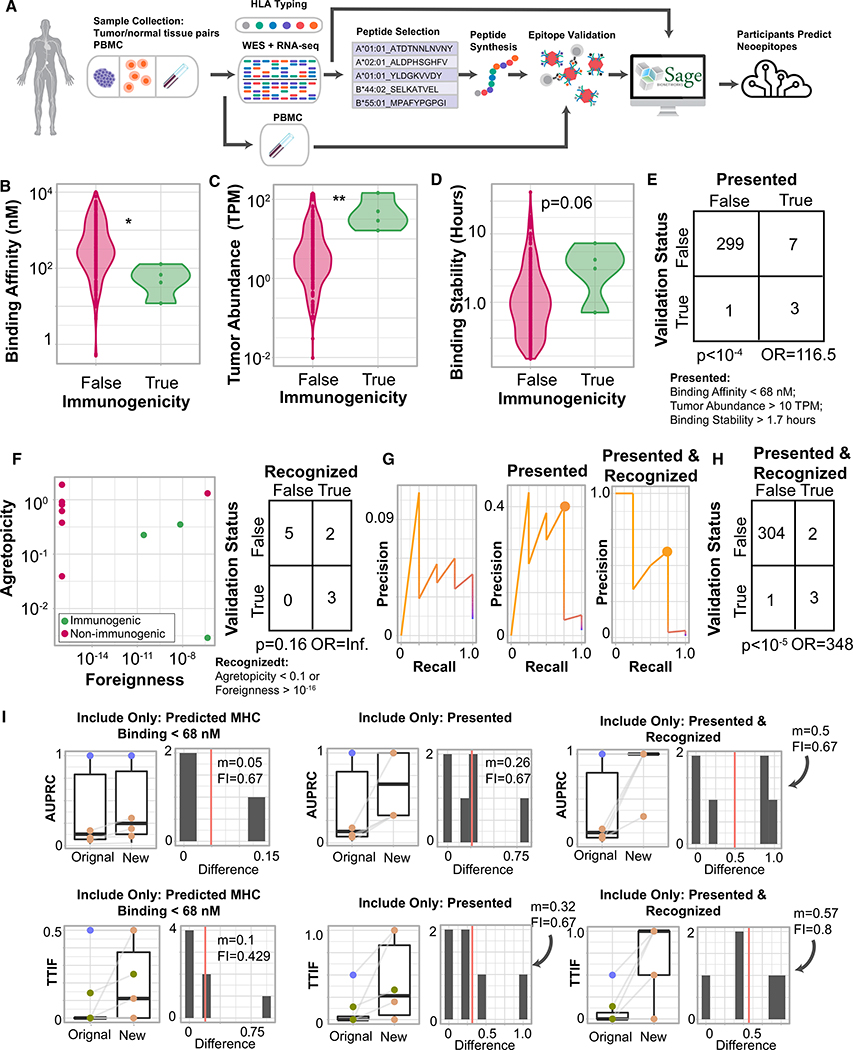
Many approaches to identify therapeutically relevant neoantigens couple tumor sequencing with bioinformatic algorithms and inferred rules of tumor epitope immunogenicity. However, there are no reference data to compare these approaches, and the parameters governing tumor epitope immunogenicity remain unclear. Here, we assembled a global consortium wherein each participant predicted immunogenic epitopes from shared tumor sequencing data. 608 epitopes were subsequently assessed for T cell binding in patient-matched samples. By integrating peptide features associated with presentation and recognition, we developed a model of tumor epitope immunogenicity that filtered out 98% of non-immunogenic peptides with a precision above 0.70. Pipelines prioritizing model features had superior performance, and pipeline alterations leveraging them improved prediction performance. These findings were validated in an independent cohort of 310 epitopes prioritized from tumor sequencing data and assessed for T cell binding. This data resource enables identification of parameters underlying effective anti-tumor immunity and is available to the research community.
Keywords: TESLA; epitope; immunogenicity; immunogenomics; immunotherapy; neoantigen.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests D.K.W. is a paid scientific advisor and shareholder in Immunai and receives research support from Bristol-Myers Squibb. M.M.v.B. is a stockholder and employee of BioNTech. V.M.H.-L. is an unpaid scientific advisor and holds equity in FX Biopharma. B.C.-A. has a contract grant with Kite Pharma and is a member of the Institutional Biosafety Committee (IBC) at Advarra Inc. N.H. is a stockholder in BioNTech, K.M.C. is a stockholder in Geneoscopy. J.Z. is an equity/stock holder and consultant to PACT Pharma. A.R. has received honoraria from consulting with Amgen, Bristol-Myers Squibb, Chugai, Genentech, Merck, Novartis, and Roche, is or has been a member of the scientific advisory board, and holds stock in Advaxis, Arcus Biosciences, Bioncotech Therapeutics, Compugen, CytomX, Five Prime, FLX-Bio, ImaginAb, Isoplexis, Kite-Gilead, Lutris Pharma, Merus, PACT Pharma, Rgenix, and Tango Therapeutics. M.D.H. receives research support from Bristol-Myers Squibb, has been a compensated consultant for Merck, Bristol-Myers Squibb, AstraZeneca, Genentech/Roche, Nektar, Syndax, Mirati, Shattuck Labs, Immunai, Blueprint Medicines, Achilles, and Arcus, received travel support/honoraria from AstraZeneca, Eli Lilly, and Bristol-Myers Squibb, has options from Shattuck Labs, Immunai, and Arcus, and has a patent filed by his institution related to the use of tumor mutation burden to predict response to immunotherapy (PCT/US2015/062208), which has received licensing fees from PGDx. P.K. is a consultant for Neon Therapeutics and Personalis. J.R.H. is board member and founder of Isoplexis and board member and founder of PACT. F.R. is an advisor/consultant to Equillium Bio, Good Therapeutics, SelectION, Inc., Cascade Drug Development Group, aTyr Pharma, and Lumos Pharma, and is a founder and holds equity in Sonoma Biotherapeutics. R.D.S. is a cofounder, scientific advisory board member, stockholder, and royalty recipient of Jounce Therapeutics and Neon Therapeutics and is a scientific advisory board member for A2 Biotherapeutics, BioLegend, Codiak Biosciences, Constellation Pharmaceuticals, NGM Biopharmaceuticals, and Sensei Biotherapeutics. J.S. and A.S. receive funding from BMS and Gritstone, are consultants for Turnstone, and perform fee-for-service assays for Neon. A.S. is a consultant for Gritstone. N.B. receives research funds from Novocure, Celldex, Ludwig institute, Genentech, Oncovir, Melanoma Research Alliance, Cancer Research Institute, Leukemia & Lymphoma Society, 485, NYSTEM, and Regeneron, and is on the advisory boards of Neon, Tempest, Checkpoint Sciences, Curevac, Primevax, Novartis, Array BioPharma, Roche, and Avidea. T.N.S. receives research funds from Merck KGaA, is consultant/advisory board member for Adaptive Biotechnologies, AIMM Therapeutics, Allogene Therapeutics, Merus, Neogene Therapeutics, Neon Therapeutics, Scenic Biotech, and Third Rock Ventures, and is a stockholder in AIMM Therapeutics, Allogene Therapeutics, BioNTech, Merus, Neogene Therapeutics, Scenic Biotech, and Third Rock Ventures Fund IV and V. A.R. has received honoraria from consulting with Amgen, Bristol-Myers Squibb, Chugai, Genentech, Merck, Novartis, Roche, and Sanofi, is or has been a member of the scientific advisory board, holds stock in Advaxis, Apricity, Arcus Biosciences, Bioncotech Therapeutics, Compugen, CytomX, Five Prime, FLX-Bio, ImaginAb, Isoplexis, Kite-Gilead, Lutris Pharma, Merus, PACT Pharma, Rgenix, and Tango Therapeutics, has received research funding from Agilent and from Bristol-Myers Squibb through Stand Up to Cancer (SU2C), and has received payment for licensing a patent on non-viral T cell gene editing to Arsenal. The remaining authors declare no conflicts of interest.
Figures
Comment in
-
Strength in Numbers: Identifying Neoantigen Targets for Cancer Immunotherapy.Cell. 2020 Oct 29;183(3):591-593. doi: 10.1016/j.cell.2020.10.011. Cell. 2020. PMID: 33125888
References
-
- Abelin JG, Harjanto D, Malloy M, Suri P, Colson T, Goulding SP, Creech AL, Serrano LR, Nasir G, Nasrullah Y, et al. (2019). Defining HLA-II Ligand Processing and Binding Rules with Mass Spectrometry Enhances Cancer Epitope Prediction. Immunity 51, 766–779. - PubMed
-
- Andersen RS, Kvistborg P, Frøsig TM, Pedersen NW, Lyngaa R, Bakker AH, Shu CJ, Straten Pt., Schumacher TN, and Hadrup SR (2012). Parallel detection of antigen-specific T cell responses by combinatorial encoding of MHC multimers. Nat. Protoc 7, 891–902. - PubMed
-
- Balachandran VP, Łuksza M, Zhao JN, Makarov V, Moral JA, Remark R, Herbst B, Askan G, Bhanot U, Senbabaoglu Y, et al. ; Australian Pancreatic Cancer Genome Initiative; Garvan Institute of Medical Research; Prince of Wales Hospital; Royal North Shore Hospital; University of Glasgow; St Vincent’s Hospital; QIMR Berghofer Medical Research Institute; University of Melbourne, Centre for Cancer Research; University of Queensland, Institute for Molecular Bioscience; Bankstown Hospital; Liverpool Hospital; Royal Prince Alfred Hospital, Chris O’Brien Lifehouse; Westmead Hospital; Fremantle Hospital; St John of God Healthcare; Royal Adelaide Hospital; Flinders Medical Centre; Envoi Pathology; Princess Alexandria Hospital; Austin Hospital; Johns Hopkins Medical Institutes; ARC-Net Centre for Applied Research on Cancer (2017). Identification of unique neoantigen qualities in long-term survivors of pancreatic cancer. Nature 551, 512–516. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
