

An observational study identifying highly tuberculosis-exposed, HIV-1-positive but persistently TB, tuberculin and IGRA negative persons with M. tuberculosis specific antibodies in Cape Town, South Africa
- PMID: 33038764
- PMCID: PMC7648124
- DOI: 10.1016/j.ebiom.2020.103053
An observational study identifying highly tuberculosis-exposed, HIV-1-positive but persistently TB, tuberculin and IGRA negative persons with M. tuberculosis specific antibodies in Cape Town, South Africa
Abstract
Background: Mycobacterium tuberculosis (Mtb) infection is inferred from positive results of T-cell immune conversion assays measuring Mtb-specific interferon gamma production or tuberculin skin test (TST) reactivity. Certain exposed individuals do not display T-cell immune conversion in these assays and do not develop TB. Here we report a hitherto unknown form of this phenotype: HIV-1-positive persistently TB, tuberculin and IGRA negative (HITTIN).
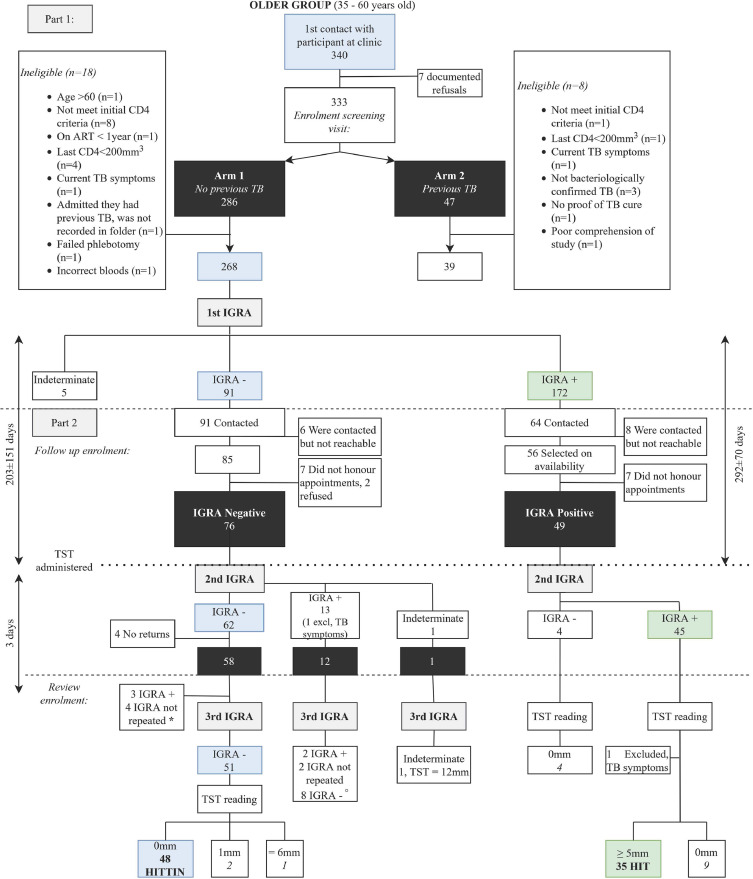
Methods: A community-based case-control design was used to systematically screen and identify adults living with HIV (HIV+), aged 35-60 years, who met stringent study criteria, and then longitudinally followed up for repeat IGRA and TST testing. Participants had no history of TB despite living in TB hyper-endemic environments in Cape Town, South Africa with a provincial incidence of 681/100,000. Mtb-specific antibodies were measured using ELISA and Luminex.
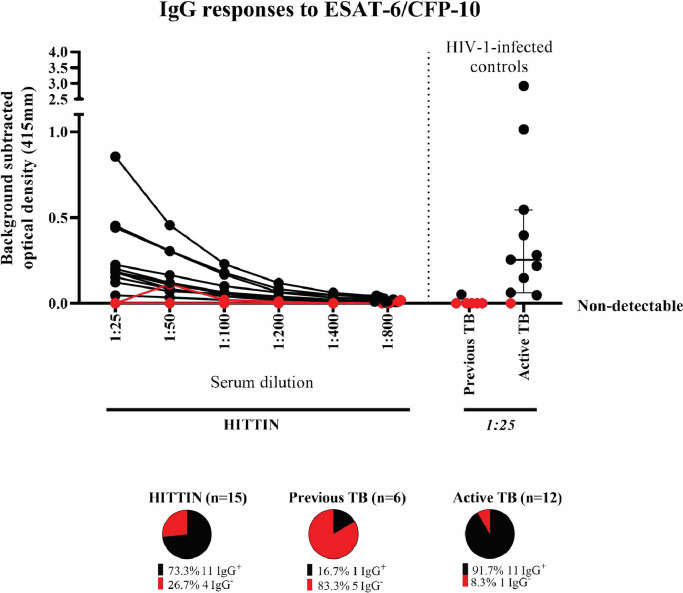
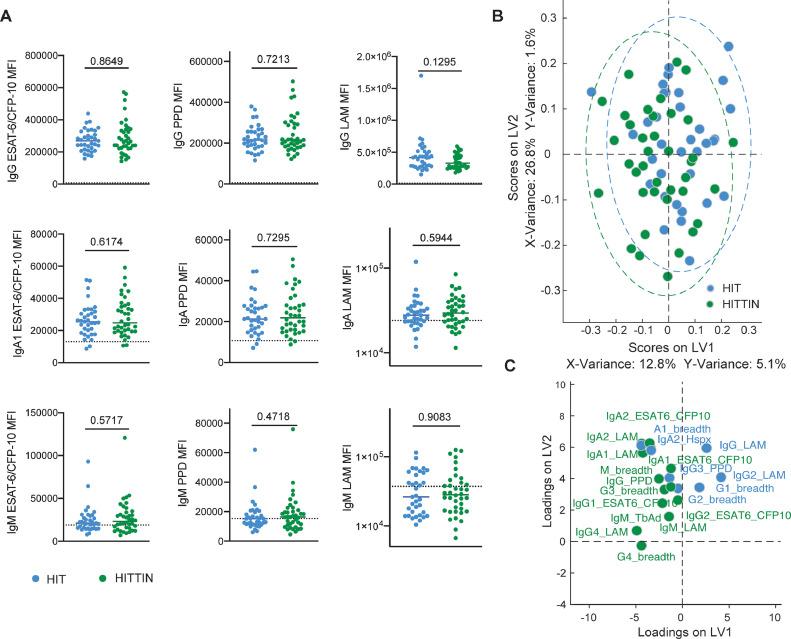
Findings: We identified 48/286 (17%) individuals who tested persistently negative for Mtb-specific T-cell immunoreactivity (three negative Quantiferon results and one TST = 0mm) over 206±154 days on average. Of these, 97·2% had documented CD4 counts<200 prior to antiretroviral therapy (ART). They had received ART for 7·0±3·0 years with a latest CD4 count of 505·8±191·4 cells/mm3. All HITTIN sent for further antibody testing (n=38) displayed Mtb-specific antibody titres.
Interpretation: Immune reconstituted HIV+ persons can be persistently non-immunoreactive to TST and interferon-γ T-cell responses to Mtb, yet develop species-specific antibody responses. Exposure is evidenced by Mtb-specific antibody titres. Our identification of HIV+ individuals displaying a persisting lack of response to TST and IGRA T-cell immune conversion paves the way for future studies to investigate this phenotype in the context of HIV-infection that so far have received only scant attention.
Keywords: Antibodies; Early clearance; Interferon gamma release assay; Resister; Tuberculin skin test.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest Data is available on reasonable request to the corresponding author. Dr Moller reports grants from National Institutes of Health, during the conduct of the study. Dr. Schurr reports to be the PI on NIH 1R01AI124349. The study was also partly funded by the Canadian Institutes of Health Research (CIHR) through grant FDN-143332 for which Dr. Schurr is the PI. Dr Kroon reports grants from National Institutes of Health, other from European and Developing Countries Clinical Trials Partnership, other from South African Medical Research Council during the conduct of the study. Dr Alter reports other from Seromyx Systems Inc outside the submitted work. In addition, Dr. Alter has a patent Systems Serology pending to Galit Alter. Dr. Wilkinson reports grants from Wellcome, grants from UK Research and Innovation, grants from Cancer Research UK, grants from National Institutes of Health, during the conduct of the study. Dr Walzl, Dr Hoal, Prof Kinnear, Dr Boolay, Dr Fischinger, Dr Orlova, Dr Jacobs and Ms Shin have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
