

Comparative Safety and Effectiveness of Vedolizumab to Tumor Necrosis Factor Antagonist Therapy for Ulcerative Colitis
- PMID: 33039584
- PMCID: PMC8026779
- DOI: 10.1016/j.cgh.2020.10.003
Comparative Safety and Effectiveness of Vedolizumab to Tumor Necrosis Factor Antagonist Therapy for Ulcerative Colitis
Abstract
Background & aims: We aimed to compare safety and effectiveness of vedolizumab to tumor necrosis factor (TNF)-antagonist therapy in ulcerative colitis in routine practice.
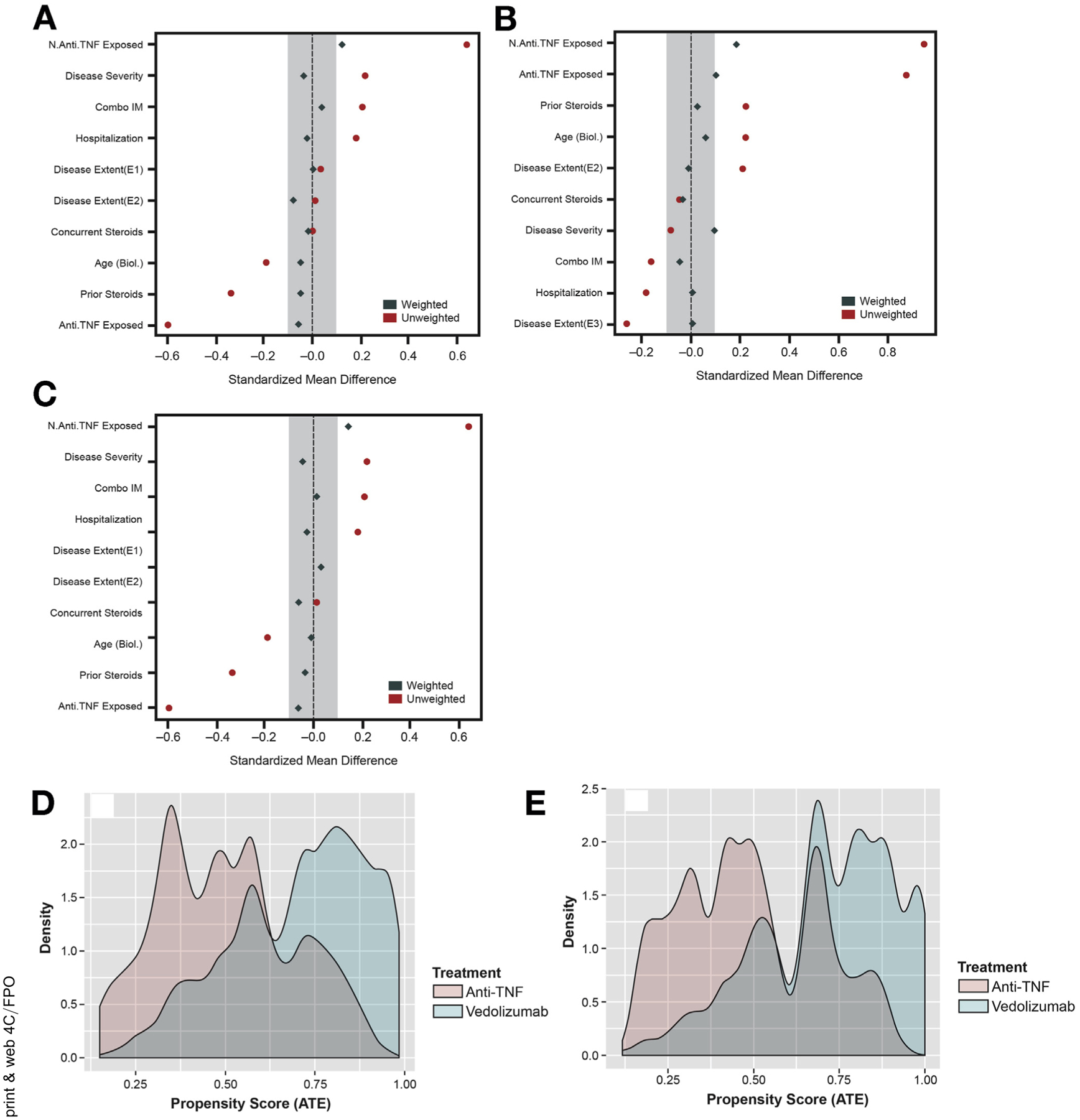
Methods: A multicenter, retrospective, observational cohort study (May 2014 to December 2017) of ulcerative colitis patients treated with vedolizumab or TNF-antagonist therapy. Propensity score weighted comparisons for development of serious adverse events and achievement of clinical remission, steroid-free clinical remission, and steroid-free deep remission. A priori determined subgroup comparisons in TNF-antagonist-naïve and -exposed patients, and for vedolizumab against infliximab and subcutaneous TNF-antagonists separately.
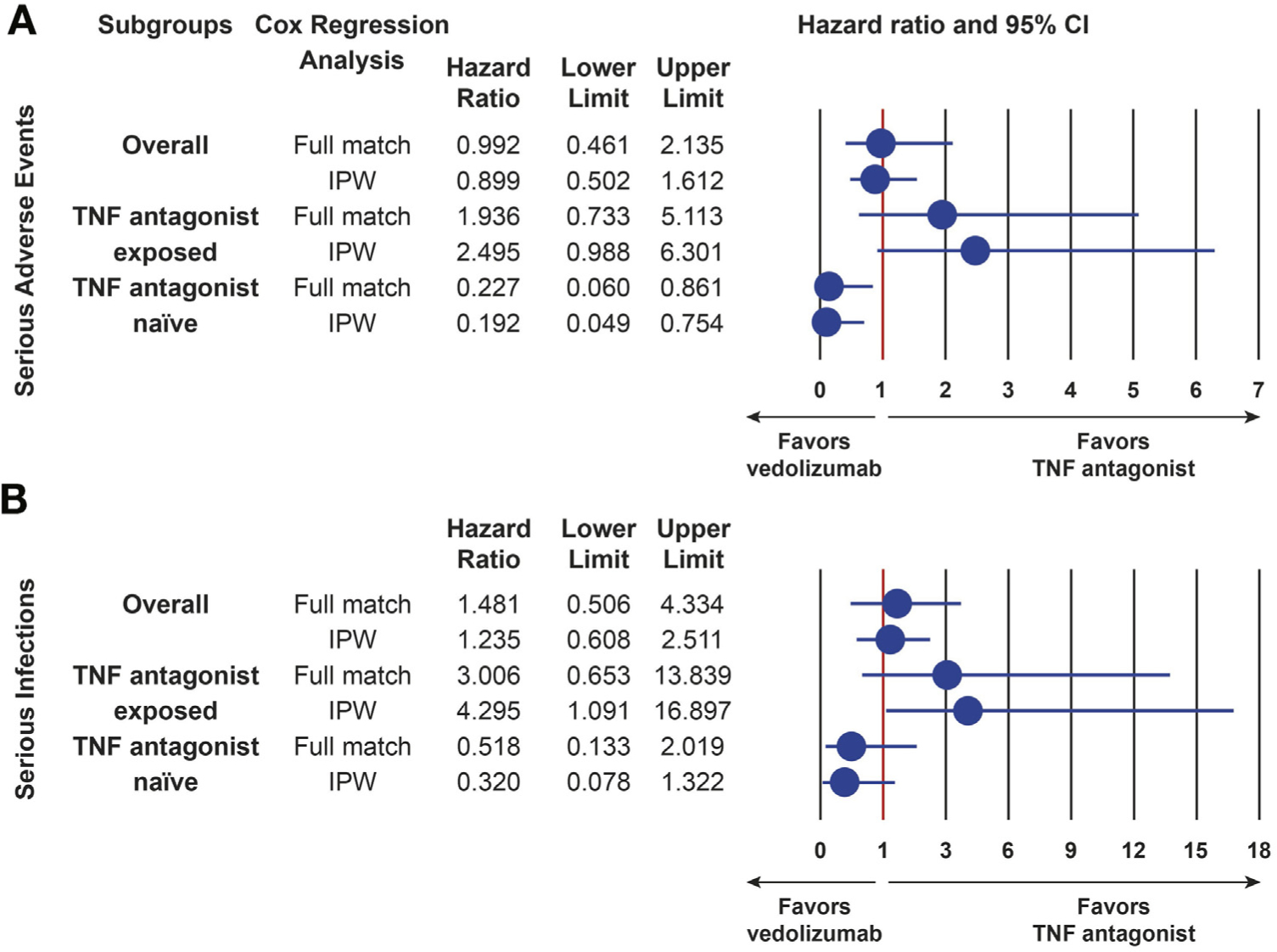
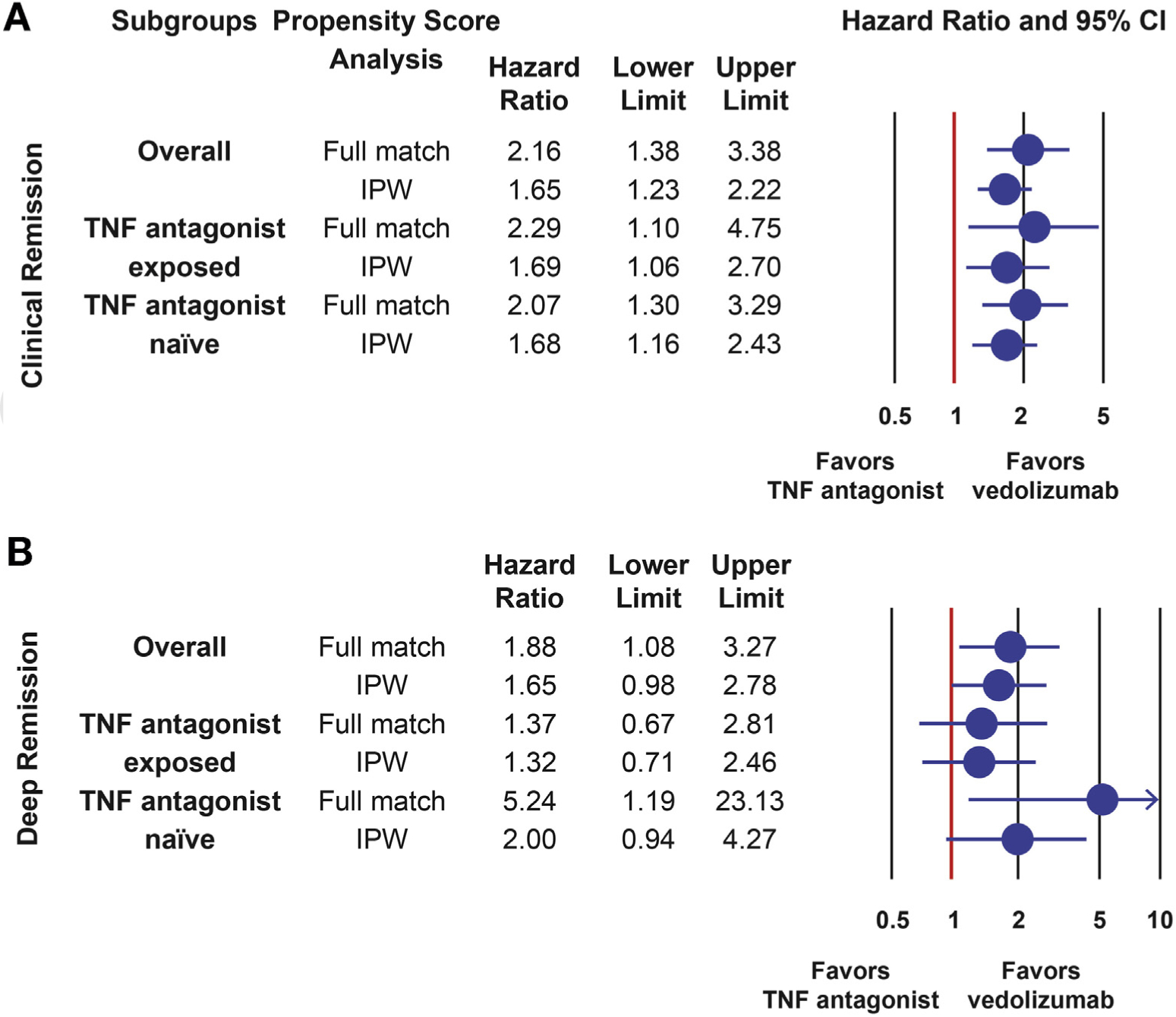
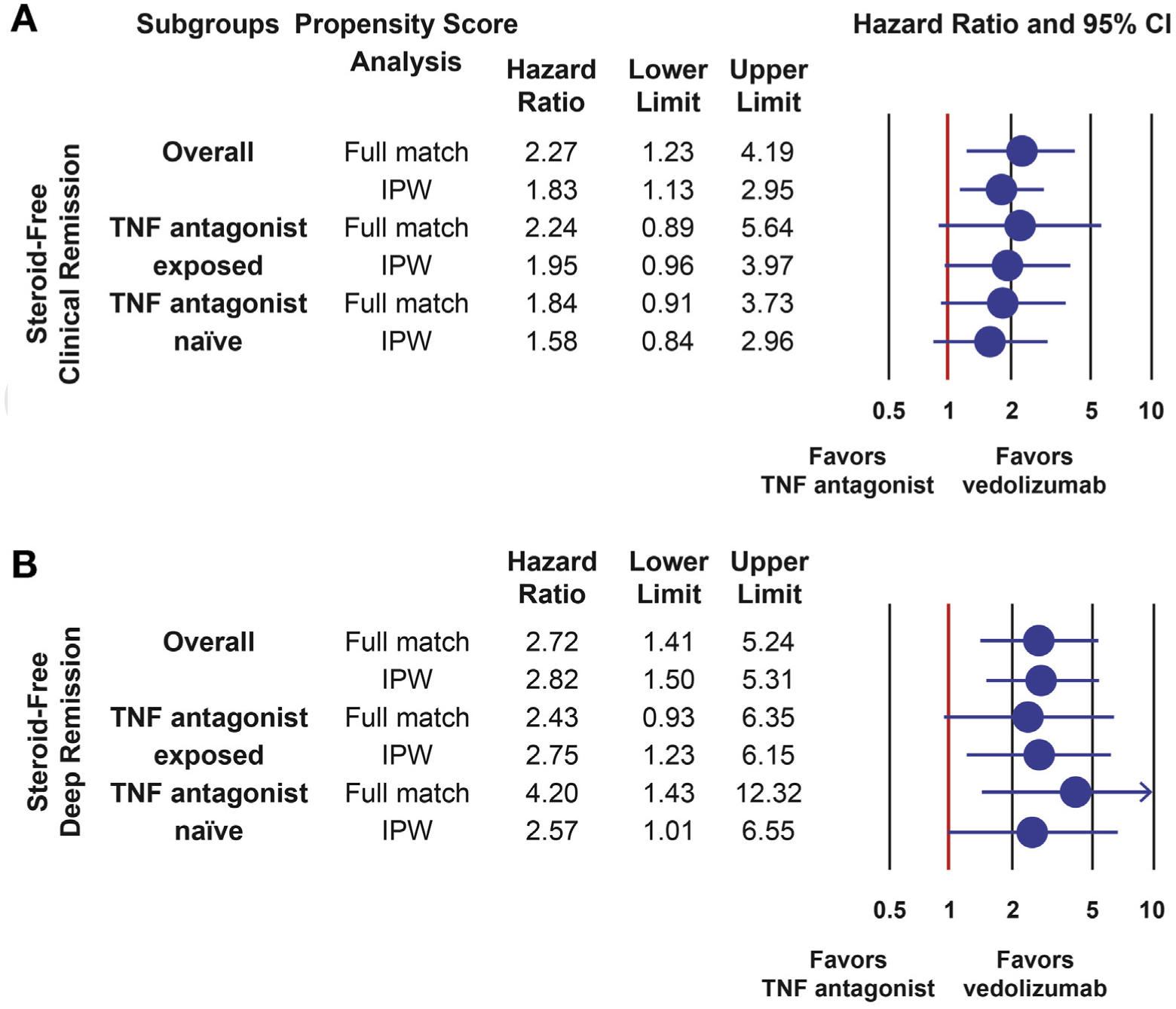
Results: A total of 722 (454 vedolizumab, 268 TNF antagonist) patients were included. Vedolizumab-treated patients were more likely to achieve clinical remission (hazard ratio [HR], 1.651; 95% confidence interval [CI], 1.229-2.217), steroid-free clinical remission (HR, 1.828; 95% CI, 1.135-2.944), and steroid-free deep remission (HR, 2.819; 95% CI, 1.496-5.310) than those treated with TNF antagonists. Results were consistent across subgroup analyses in TNF-antagonist-naïve and -exposed patients, and for vedolizumab vs infliximab and vs subcutaneous TNF-antagonist agents separately. Overall, there were no statistically significant differences in the risk of serious adverse events (HR, 0.899; 95% CI, 0.502-1.612) or serious infections (HR, 1.235; 95% CI, 0.608-2.511) between vedolizumab-treated and TNF-antagonist-treated patients. However, in TNF-antagonist-naïve patients, vedolizumab was less likely to be associated with serious adverse events than TNF antagonists (HR, 0.192; 95% CI, 0.049-0.754).
Conclusions: Treatment of ulcerative colitis with vedolizumab is associated with higher rates of remission than treatment with TNF-antagonist therapy in routine practice, and lower rates of serious adverse events in TNF-antagonist-naïve patients.
Keywords: Biologics; Comparative Research; Health Outcomes.
Copyright © 2022. Published by Elsevier Inc.
Figures
References
-
- Mao EJ, Hazlewood GS, Kaplan GG, et al. Systematic review with meta-analysis: comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther 2017;45:3–13. - PubMed
-
- Bressler B, Marshall JK, Bernstein CN, et al. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the Toronto consensus. Gastroenterology 2015; 148:1035–1058.e1033. - PubMed
-
- Rubin DT, Ananthakrishnan AN, Siegal CA, et al. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol 2019; 114:384–413. - PubMed
-
- Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis: part 2—current management. J Crohns Colitis 2017;11:769–784. - PubMed
