

Exploring the pathophysiology of post-sepsis syndrome to identify therapeutic opportunities
- PMID: 33039713
- PMCID: PMC7544455
- DOI: 10.1016/j.ebiom.2020.103044
Exploring the pathophysiology of post-sepsis syndrome to identify therapeutic opportunities
Abstract
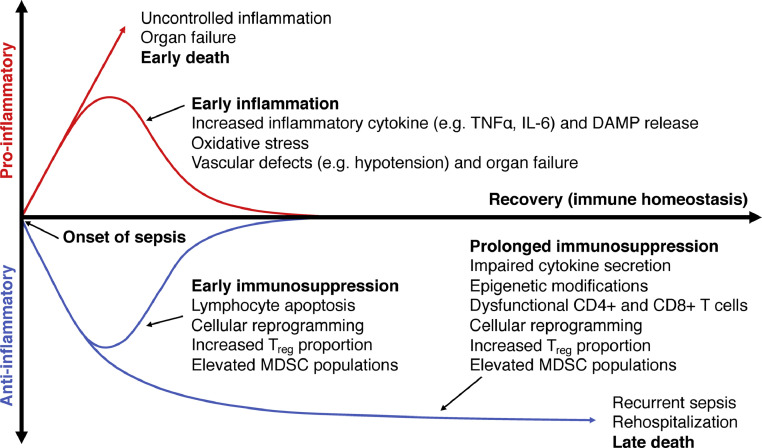
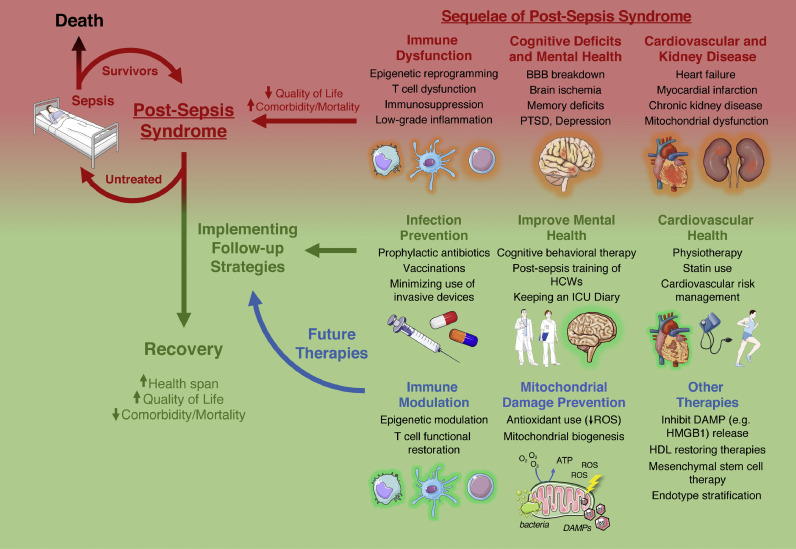
Sepsis is a major health problem worldwide. As the number of sepsis cases increases, so does the number of sepsis survivors who suffer from "post-sepsis syndrome" after hospital discharge. This syndrome involves deficits in multiple systems, including the immune, cognitive, psychiatric, cardiovascular, and renal systems. Combined, these detrimental consequences lead to rehospitalizations, poorer quality of life, and increased mortality. Understanding the pathophysiology of these issues is crucial to develop new therapeutic opportunities to improve survival rate and quality of life of sepsis survivors. Such novel strategies include modulating the immune system and addressing mitochondrial dysfunction. A sepsis follow-up clinic may be useful to identify long-term health issues associated with post-sepsis syndrome and evaluate existing and novel strategies to improve the lives of sepsis survivors.
Keywords: Post-sepsis syndrome; Quality of life; Rehospitalization; Sepsis.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Current Understanding of Long-Term Cognitive Impairment After Sepsis.Front Immunol. 2022 May 6;13:855006. doi: 10.3389/fimmu.2022.855006. eCollection 2022. Front Immunol. 2022. PMID: 35603184 Free PMC article. Review.
-
Long-Term Risk of Cardiovascular Events in Patients With Chronic Kidney Disease Who Have Survived Sepsis: A Nationwide Cohort Study.J Am Heart Assoc. 2017 Feb 10;6(2):e004613. doi: 10.1161/JAHA.116.004613. J Am Heart Assoc. 2017. PMID: 28188252 Free PMC article.
-
Characterization of Readmission by Day of Rehospitalization After Colorectal Surgery.Dis Colon Rectum. 2017 Feb;60(2):202-212. doi: 10.1097/DCR.0000000000000734. Dis Colon Rectum. 2017. PMID: 28059917
-
Development, Validation, and Clinical Utility Assessment of a Prognostic Score for 1-Year Unplanned Rehospitalization or Death of Adult Sepsis Survivors.JAMA Netw Open. 2020 Sep 1;3(9):e2013580. doi: 10.1001/jamanetworkopen.2020.13580. JAMA Netw Open. 2020. PMID: 32926114 Free PMC article.
-
Innate Immunity in the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome and Its Implications for Therapy.Front Immunol. 2018 Apr 4;9:595. doi: 10.3389/fimmu.2018.00595. eCollection 2018. Front Immunol. 2018. PMID: 29670613 Free PMC article. Review.
Cited by
-
Sepsis-associated brain injury: underlying mechanisms and potential therapeutic strategies for acute and long-term cognitive impairments.J Neuroinflammation. 2022 Apr 29;19(1):101. doi: 10.1186/s12974-022-02464-4. J Neuroinflammation. 2022. PMID: 35488237 Free PMC article. Review.
-
Understanding Post-Sepsis Syndrome: How Can Clinicians Help?Infect Drug Resist. 2023 Sep 29;16:6493-6511. doi: 10.2147/IDR.S390947. eCollection 2023. Infect Drug Resist. 2023. PMID: 37795206 Free PMC article. Review.
-
During Sepsis and COVID-19, the Pro-Inflammatory and Anti-Inflammatory Responses Are Concomitant.Clin Rev Allergy Immunol. 2023 Oct;65(2):183-187. doi: 10.1007/s12016-023-08965-1. Epub 2023 Jul 3. Clin Rev Allergy Immunol. 2023. PMID: 37395985 Review.
-
Transitional care after hospitalization for sepsis in Germany- results from the population-based AVENIR cohort study.Infection. 2025 Jul 8. doi: 10.1007/s15010-025-02589-7. Online ahead of print. Infection. 2025. PMID: 40627302
-
Long-term Mortality and Hospital Readmissions Among Survivors of Sepsis in Sweden: A Population-Based Cohort Study.Open Forum Infect Dis. 2024 Jun 24;11(7):ofae331. doi: 10.1093/ofid/ofae331. eCollection 2024 Jul. Open Forum Infect Dis. 2024. PMID: 38962525 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
