

Early indicators of disease progression in Fabry disease that may indicate the need for disease-specific treatment initiation: findings from the opinion-based PREDICT-FD modified Delphi consensus initiative
- PMID: 33039984
- PMCID: PMC7549469
- DOI: 10.1136/bmjopen-2019-035182
Early indicators of disease progression in Fabry disease that may indicate the need for disease-specific treatment initiation: findings from the opinion-based PREDICT-FD modified Delphi consensus initiative
Abstract
Objectives: The PRoposing Early Disease Indicators for Clinical Tracking in Fabry Disease (PREDICT-FD) initiative aimed to reach consensus among a panel of global experts on early indicators of disease progression that may justify FD-specific treatment initiation.
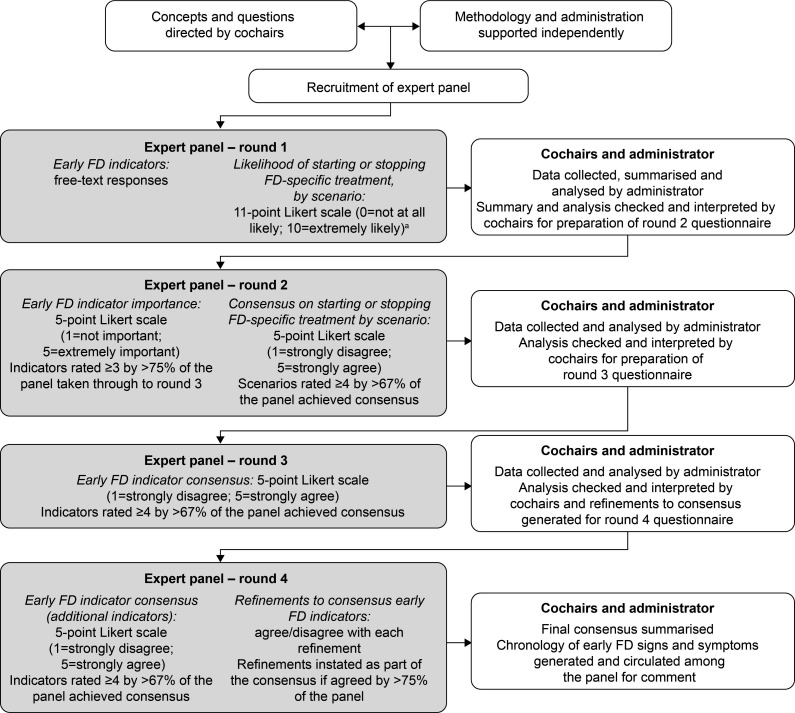
Design and setting: Anonymous feedback from panellists via online questionnaires was analysed using a modified Delphi consensus technique. Questionnaires and data were managed by an independent administrator directed by two non-voting cochairs. First, possible early indicators of renal, cardiac and central/peripheral nervous system (CNS/PNS) damage, and other disease and patient-reported indicators assessable in routine clinical practice were compiled by the cochairs and administrator from panellists' free-text responses. Second, the panel scored indicators for importance (5-point scale: 1=not important; 5=extremely important); indicators scoring ≥3 among >75% of panellists were then rated for agreement (5-point scale: 1=strongly disagree; 5=strongly agree). Indicators awarded an agreement score ≥4 by >67% of panellists achieved consensus. Finally, any panel-proposed refinements to consensus indicator definitions were adopted if >75% of panellists agreed.
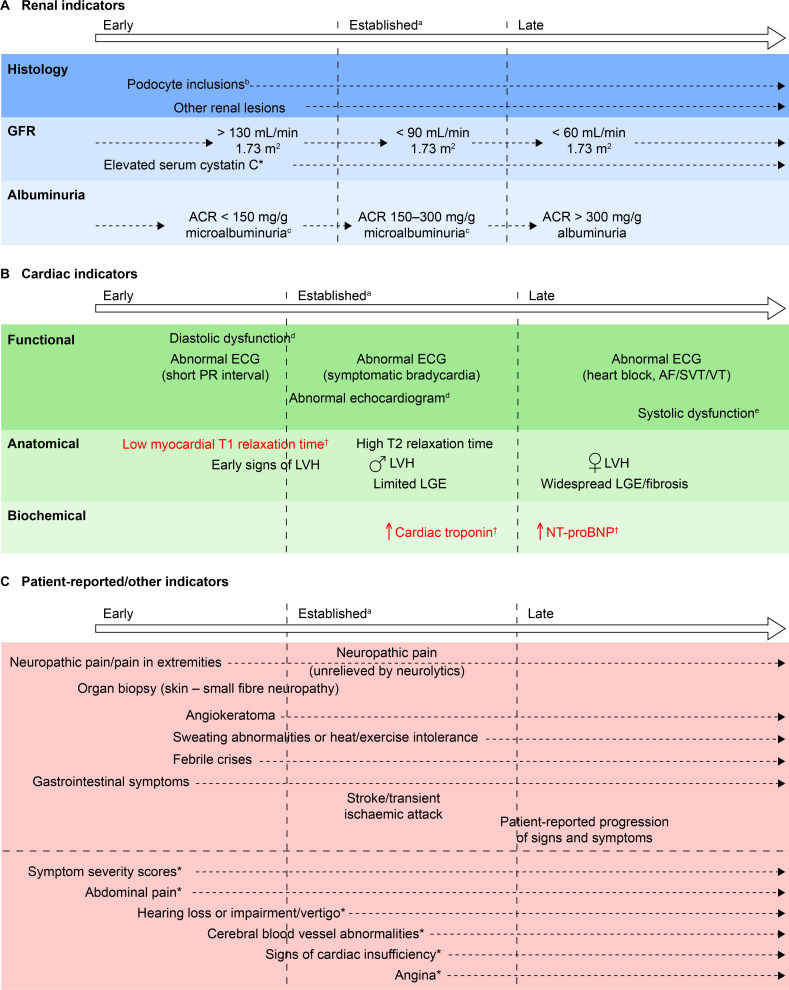
Results: A panel of 21 expert clinicians from 15 countries provided information from which 83 possible current indicators of damage (kidney, 15; cardiac, 15; CNS/PNS, 13; other, 16; patient reported, 24) were compiled. Of 45 indicators meeting the importance criteria, consensus was reached for 29 and consolidated as 27 indicators (kidney, 6; cardiac, 10; CNS/PNS, 2; other, 6; patient reported, 3) including: (kidney) elevated albumin:creatinine ratio, histological damage, microalbuminuria; (cardiac) markers of early systolic/diastolic dysfunction, elevated serum cardiac troponin; (CNS/PNS) neuropathic pain, gastrointestinal symptoms suggestive of gastrointestinal neuropathy; (other) pain in extremities/neuropathy, angiokeratoma; (patient-reported) febrile crises, progression of symptoms/signs. Panellists revised and approved proposed chronologies of when the consensus indicators manifest. The panel response rate was >95% at all stages.
Conclusions: PREDICT-FD captured global opinion regarding current clinical indicators that could prompt FD-specific treatment initiation earlier than is currently practised.
Keywords: cardiomyopathy; chronic renal failure; genetics; stroke medicine.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DAH: advisory boards for Amicus, Sanofi, Shire (now part of Takeda); consulting fees from Amicus, Idorsia, Sanofi and Shire (now part of Takeda); honoraria from Amicus, Sanofi and Shire (now part of Takeda). PA: research grant and honoraria from Shire (now part of Takeda); honoraria from Amicus, Biomarin, Sanofi and Ultragenyx. PBD: speaker honoraria from and advisory boards for Takeda and Sanofi; consultancy for Sanofi. FE: travel grants and speaker honoraria from Pfizer, Sanofi Genzyme and Takeda. AF: research grants from Amicus and Shire. OL: travel grants and speaker honoraria from Amicus, Sanofi Genzyme and Shire HGT. AL: speaker’s honoraria or consultation fees from Amicus, Sanofi Genzyme and Takeda. J-CL: speaker’s honoraria and consultation fees from Shire. JCM: research grant and speaker honoraria from Sanofi Genzyme; advisory board for, and honoraria from ST; consulting fees from 4DMT. KN: research support and/or honoraria from Amicus, Idorsia, Protalix, Sanofi and Shire (now part of Takeda); advisory boards for Amicus, Sanofi and Shire (now part of Takeda). D-MN: research funding from Shire (now part of Takeda) and Sanofi. AN: honoraria and research support from Sanofi Genzyme and Shire (now part of Takeda). UR: advisory boards for Amicus, Chiesi, Idorsia and Shire; travel grants and honoraria from Amicus, Genzyme and Shire. RR: travel grants and speaker honoraria from Amicus and Shire HGT (now part of Takeda). PR: advisory board, consulting fees and research grant from Shire (now part of Takeda). RS: advisory boards for Amicus, Sanofi, Shire (now part of Takeda); honoraria from Amicus and Shire; research funding from Idorisia, Protalix, Sanofi Genzyme and Takeda. ES: speaker’s fees and travel support from Amicus, Sanofi Genzyme and Shire; advisory board honoraria from Amicus and Sanofi Genzyme. MT: advisory boards for Amicus, Sanofi and Shire (now part of Takeda); travel grants and speaker’s honoraria from Amicus, Sanofi and Shire; research funding from Amicus, AVROBIO and Idorsia. RT: travel grants, speaker’s honoraria or consultation fees from Amicus, Sanofi Genzyme and Takeda. BV: speaker’s fees and travel support from Greenovation, Sanofi Genzyme and Shire/Takeda; advisory board honoraria from Sanofi Genzyme. DGW: advisory boards for Amicus, Avrobio, Freeline Therapeutics, 4D-MT Technology, Idorsia and Protalix; honoraria and travel expenses from Amicus, Protalix and Sanofi; and equity interest in Reata Pharmaceuticals. MLW: advisory boards for Amicus, Sanofi and Shire (now part of Takeda); honoraria from Amicus, Sanofi and Shire; research funding from Amicus, Idorisia, Protalix and Shire. JJ: honoraria from Sanofi; travel expenses from Amicus and Sanofi. MJR is an employee of Oxford PharmaGenesis (Oxford, UK). SF: advisory boards for Amicus; consulting fees from Shire (now part of Takeda); contracted research from Shire (now part of Takeda); honoraria from Amicus, Sanofi and Shire (now part of Takeda); speaker’s bureau for Amicus, Sanofi and Shire (now part of Takeda); travel expenses from Amicus, Sanofi and Shire (now part of Takeda).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical