

Placental site trophoblastic tumour: the rarest subtype of gestational trophoblastic disease
- PMID: 33040035
- PMCID: PMC7552802
- DOI: 10.1136/bcr-2020-235756
Placental site trophoblastic tumour: the rarest subtype of gestational trophoblastic disease
Abstract
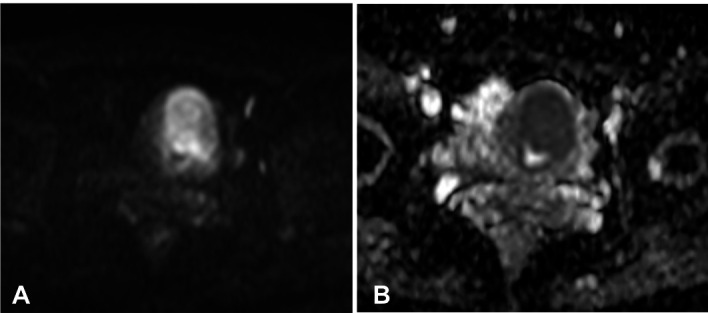
Placental site trophoblastic tumour (PSTT) is a very rare form of gestational trophoblastic disease that grows slowly, secretes low levels of beta-subunit of human chorionic gonadotropin (β-hCG), presents late-onset metastatic potential and is resistant to several chemotherapy regimens. Here, we report a case of PSTT in a 36-year-old woman who presented with amenorrhea and persistently elevated serum level of β-hCG after a miscarriage. Transvaginal ultrasound revealed a hypovascular ill-defined solid lesion of the uterine fundus and MRI showed a tumour infiltrating the external myometrium with discrete early enhancement and signal restriction on diffusion-weighted imaging. PSTT was suspected, and after endometrial biopsy by hysteroscopy and posterior hysterectomy, microscopic examination allowed the final diagnosis. The level of β-hCG dropped significantly in about a month after surgical treatment. Due to the rarity of PSTT, reporting new cases is crucial to improve the diagnosis and managing of these patients.
Keywords: gynecological cancer; pathology; radiology.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





Similar articles
-
Gestational trophoblastic diseases: 3. Human chorionic gonadotropin-free beta-subunit, a reliable marker of placental site trophoblastic tumors.Gynecol Oncol. 2006 Aug;102(2):160-4. doi: 10.1016/j.ygyno.2005.12.046. Epub 2006 May 2. Gynecol Oncol. 2006. PMID: 16631918
-
Placental site trophoblastic tumor, report of a case with unusual presentation.Placenta. 2013 May;34(5):460-2. doi: 10.1016/j.placenta.2013.01.010. Epub 2013 Mar 9. Placenta. 2013. PMID: 23478075
-
A first stage placental site trophoblastic tumor: a case report and review of literature.Minerva Obstet Gynecol. 2022 Dec;74(6):542-548. doi: 10.23736/S2724-606X.22.05053-9. Epub 2022 Mar 2. Minerva Obstet Gynecol. 2022. PMID: 35238194 Review.
-
[Diagnosis and therapeutics of placental site trophoblastic tumor].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2002 Aug;24(4):418-21. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2002. PMID: 12905666 Chinese.
-
Placental site trophoblastic tumor: a case report and review of the literature.J Radiol Case Rep. 2015 Apr 30;9(4):14-22. doi: 10.3941/jrcr.v9i4.2146. eCollection 2015 Apr. J Radiol Case Rep. 2015. PMID: 26622924 Free PMC article. Review.
Cited by
-
Gestational trophoblastic disease: an update.Abdom Radiol (NY). 2023 May;48(5):1793-1815. doi: 10.1007/s00261-023-03820-5. Epub 2023 Feb 10. Abdom Radiol (NY). 2023. PMID: 36763119 Review.
-
Additional value of uterine artery Doppler pulsatility index for ultrasound diagnosis of placental site trophoblastic tumor: prospective cohort study.Ultrasound Obstet Gynecol. 2025 Jul;66(1):73-80. doi: 10.1002/uog.29235. Epub 2025 May 19. Ultrasound Obstet Gynecol. 2025. PMID: 40387112 Free PMC article.
-
Advances in the diagnosis and early management of gestational trophoblastic disease.BMJ Med. 2022 Dec 16;1(1):e000321. doi: 10.1136/bmjmed-2022-000321. eCollection 2022. BMJ Med. 2022. PMID: 36936581 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical