

A model-based cost-effectiveness analysis of pharmacogenomic panel testing in cardiovascular disease management: preemptive, reactive, or none?
- PMID: 33041335
- PMCID: PMC7935716
- DOI: 10.1038/s41436-020-00995-w
A model-based cost-effectiveness analysis of pharmacogenomic panel testing in cardiovascular disease management: preemptive, reactive, or none?
Abstract
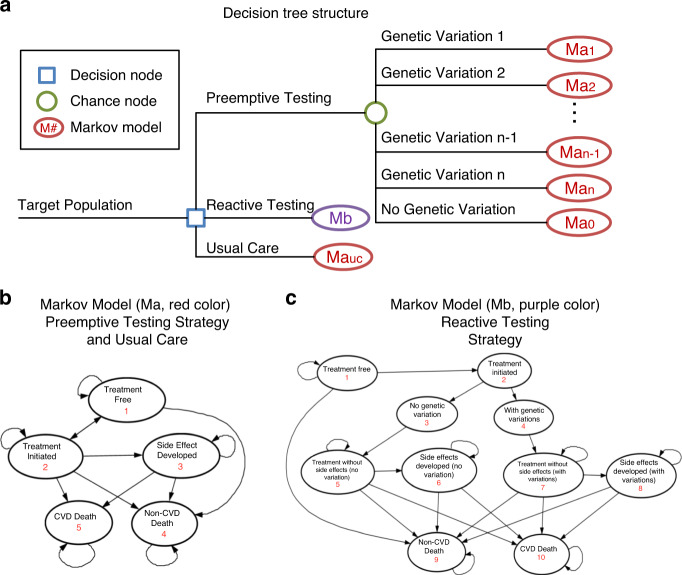
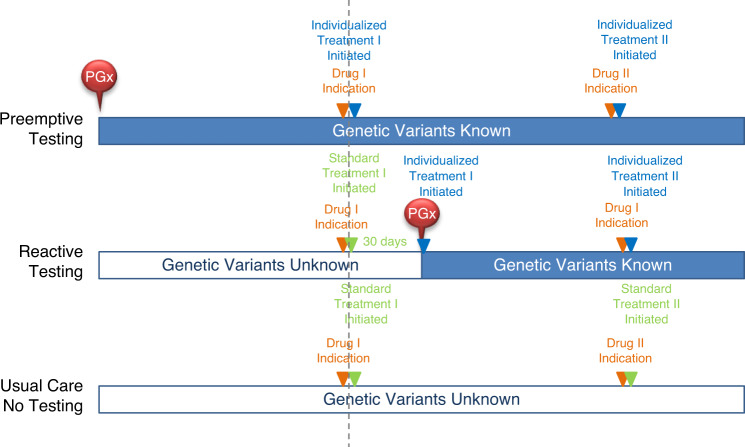
Purpose: Pharmacogenomics (PGx) studies how inherited genetic variations in individuals affect drug absorption, distribution, and metabolism. PGx panel testing can potentially help improve efficiency and accuracy in individualizing therapy. This study compared the cost-effectiveness between preemptive PGx panel testing, reactive PGx panel testing and usual care (no testing) in cardiovascular disease management.
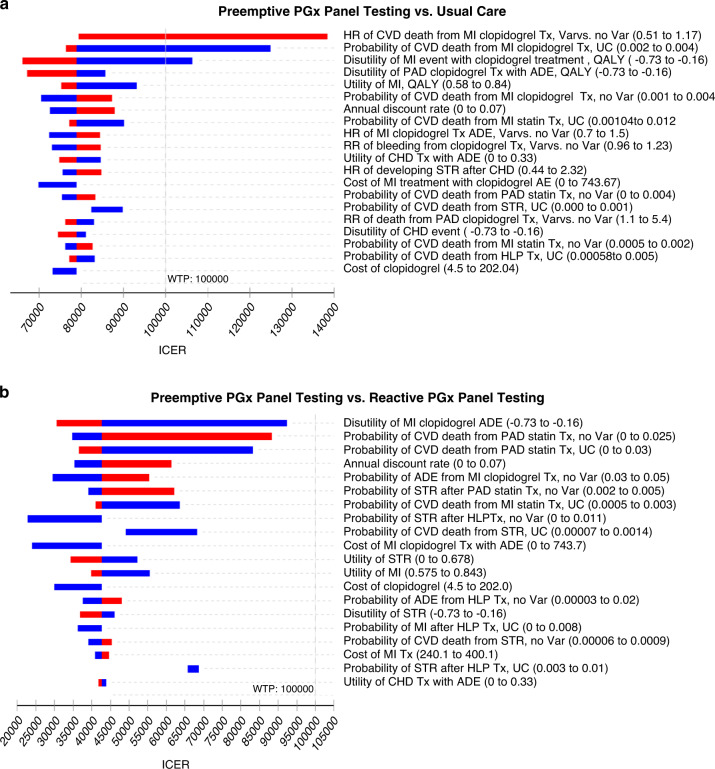
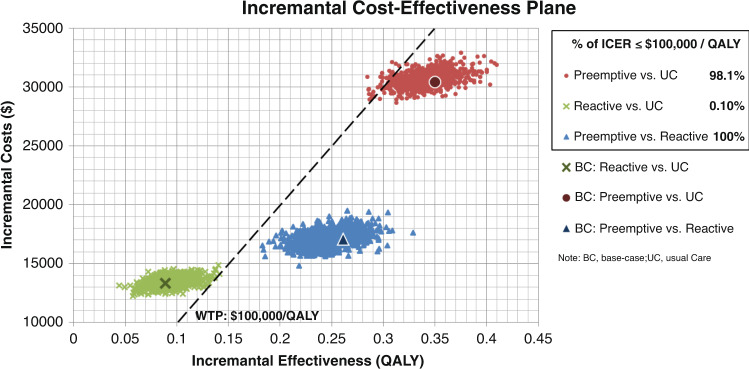
Methods: We developed a decision analytic model from the US payer's perspective for a hypothetical cohort of 10,000 patients ≥45 years old, using a short-term decision tree and long-term Markov model. The testing panel included the following gene-drug pairs: CYP2C19-clopidogrel, CYP2C9/VKORC1-warfarin, and SLCO1B1-statins with 30 test-return days. Costs were reported in 2019 US dollars and effectiveness was measured in quality-adjusted life years (QALYs). The primary outcome was incremental cost-effectiveness ratio (ICER = ΔCost/ΔQALY), assuming 3% discount rate for costs and QALYs. Scenario and probabilistic sensitivity analyses were performed to assess the impact of demographics, risk level, and follow-up timeframe.
Results: Preemptive testing was found to be cost-effective compared with usual care (ICER $86,227/QALY) at the willingness-to-pay threshold of $100,000/QALY while reactive testing was not (ICER $148,726/QALY). Sensitivity analyses suggested that our cost-effectiveness results were sensitive to longer follow-up, and the age group 45-64 years.
Conclusion: Compared with usual care, preemptive PGx panel testing was cost-effective in cardiovascular disease management.
Keywords: cardiovascular diseases management; cost-effectiveness; genomic panel testing; pharmacogenomics.
Conflict of interest statement
R.W. and L.W. are cofounders of and stockholders in OneOme LLC, a pharmacogenomic decision support company. The other authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
