

Stress and Tinnitus; Transcutaneous Auricular Vagal Nerve Stimulation Attenuates Tinnitus-Triggered Stress Reaction
- PMID: 33041937
- PMCID: PMC7527536
- DOI: 10.3389/fpsyg.2020.570196
Stress and Tinnitus; Transcutaneous Auricular Vagal Nerve Stimulation Attenuates Tinnitus-Triggered Stress Reaction
Abstract
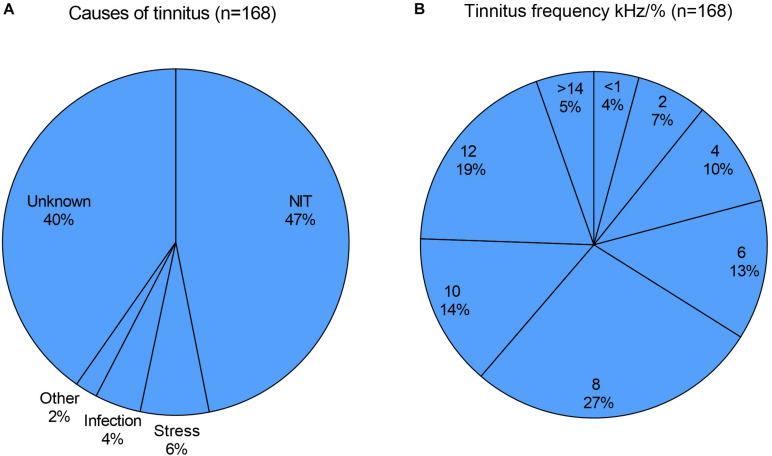
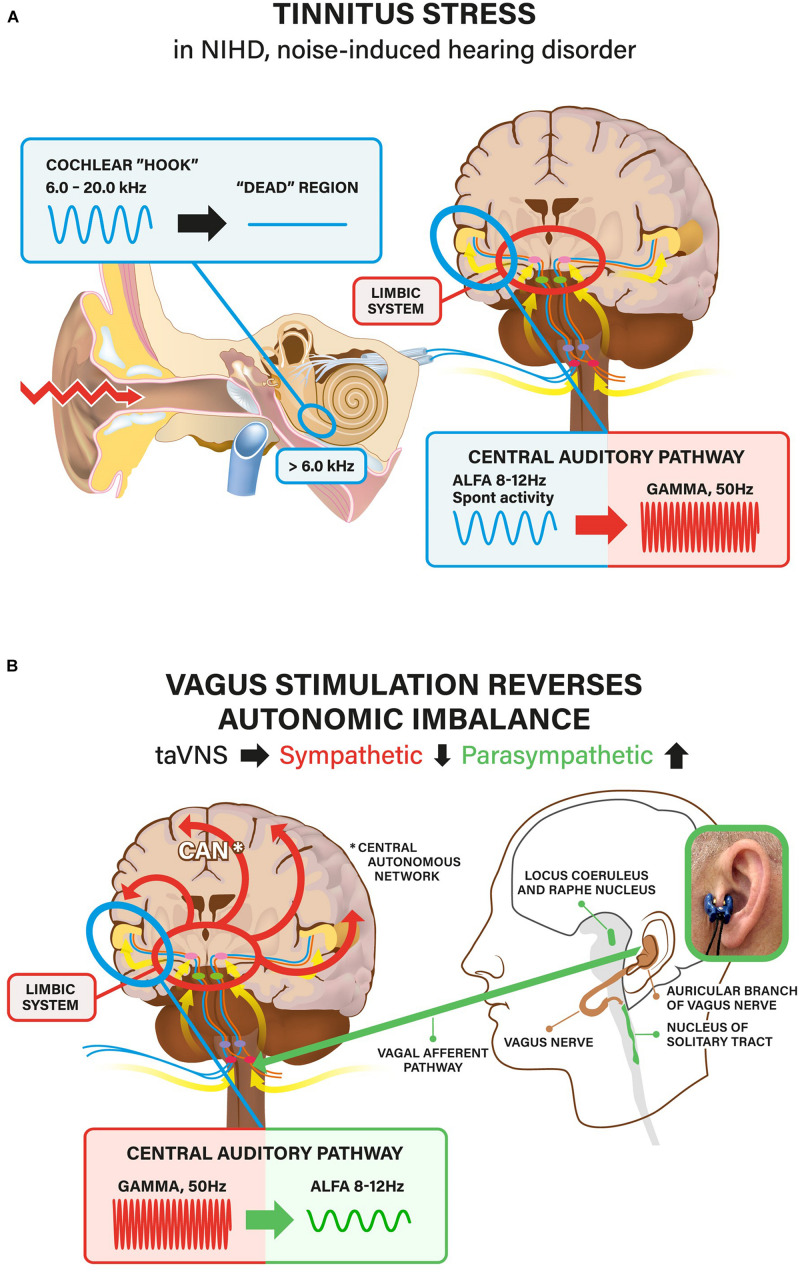
Introduction: Tinnitus can become a strong stressor for some individuals, leading to imbalance of the autonomous nervous system with reduction of parasympathetic activity. It can manifest itself as sleep disturbances, anxiety and even depression. This condition can be reversed by bioelectrical vagal nerve stimulation (VNS). Conventional invasive VNS is an approved treatment for epilepsy and depression. Transcutaneous VNS (taVNS) stimulating the auricular branch of the vagus nerve has been shown to activate the vagal pathways similarly as an implanted VNS. Therefore, taVNS might also be a therapeutic alternative in health conditions such as tinnitus-related mental stress (TRMS). This retrospective study in 171 TRMS patients reports the clinical features, psychophysiological characteristics, and results of the heart rate variability (HRV) tests before and after test-taVNS. This study also reports the therapy outcomes of 113 TRMS patients treated with taVNS, in combination with standard tinnitus therapy.
Methods: Diagnostic tinnitus and hearing profiles were defined. To detect possible cardiac adverse effects, test-taVNS with heart rate monitoring as well as pre- and post-stimulation HRV tests were performed. Daily taVNS home therapy was prescribed thereafter. To assess therapeutic usefulness of taVNS, 1-year follow-up outcome was studied. Results of HRV tests were retrospectively analyzed and correlated to diagnostic data.
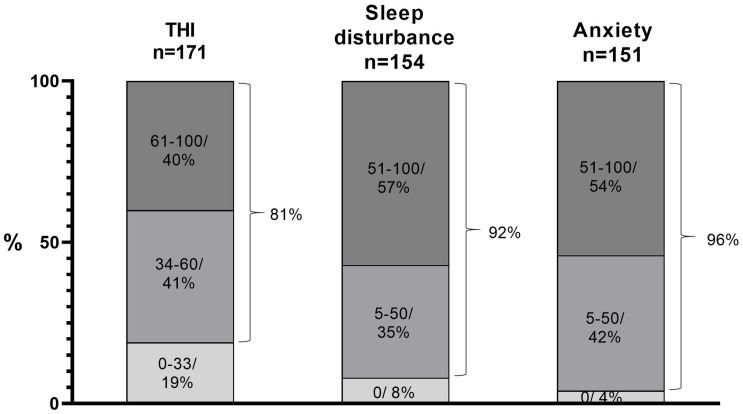
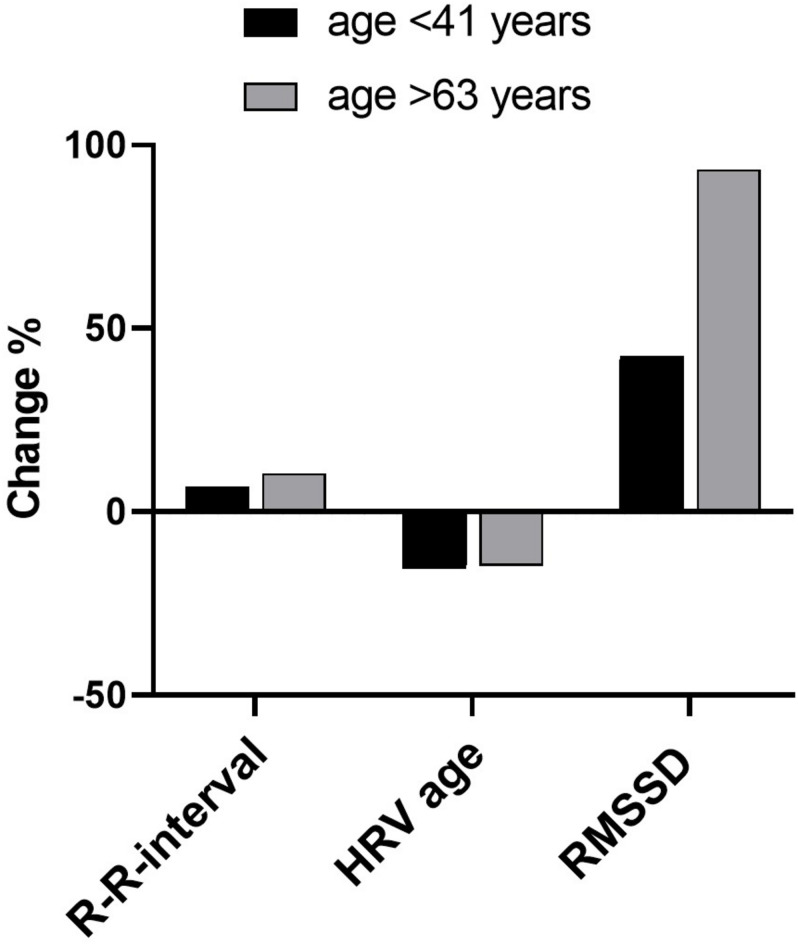
Results: The large majority of patients with TRMS suffer from associated symptoms such as sleep disturbances and anxiety. Baseline HRV data showed that more than three quarters of the 171 patients had increased sympathetic activity before test-taVNS. Test-taVNS shifted mean values of different HRV parameters toward increased parasympathetic activity in about 80% of patients. Test-taVNS did not cause any cardiac or other side effects. No significant adverse effects were reported in follow-up questionnaires.
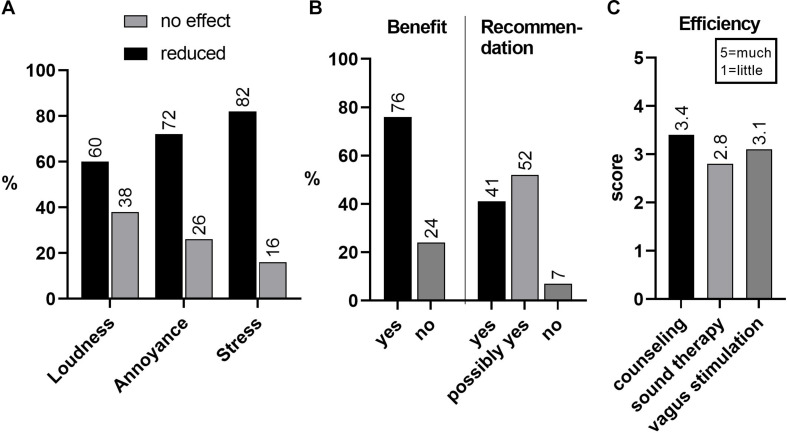
Conclusion: TRMS is an example of a stress condition in which patients may benefit from taVNS. As revealed by HRV, test-taVNS improved parasympathetic function, most efficiently in patients with a low starting HRV level. Our tinnitus treatment program, including taVNS, effectively alleviated tinnitus stress and handicap. For wider clinical use, there is a great need for more knowledge about the optimal methodology and parameters of taVNS.
Keywords: neuromodulation; parasympathetic; patients; stress; tinnitus; vagus.
Copyright © 2020 Ylikoski, Markkanen, Pirvola, Lehtimäki, Ylikoski, Jing, Sinkkonen and Mäkitie.
Figures

Similar articles
-
Ear your heart: transcutaneous auricular vagus nerve stimulation on heart rate variability in healthy young participants.PeerJ. 2022 Nov 21;10:e14447. doi: 10.7717/peerj.14447. eCollection 2022. PeerJ. 2022. PMID: 36438582 Free PMC article.
-
Non-Invasive Auricular Vagus Nerve Stimulation Decreases Heart Rate Variability Independent of Caloric Load.Psychophysiology. 2025 Feb;62(2):e70017. doi: 10.1111/psyp.70017. Psychophysiology. 2025. PMID: 40007175 Free PMC article. Clinical Trial.
-
Neuro-cardiac coupling predicts transcutaneous auricular vagus nerve stimulation effects.Brain Stimul. 2021 Mar-Apr;14(2):209-216. doi: 10.1016/j.brs.2021.01.001. Epub 2021 Jan 7. Brain Stimul. 2021. PMID: 33422683
-
Transcutaneous auricular vagus nerve stimulators: a review of past, present, and future devices.Expert Rev Med Devices. 2022 Jan;19(1):43-61. doi: 10.1080/17434440.2022.2020095. Epub 2022 Jan 13. Expert Rev Med Devices. 2022. PMID: 34937487 Review.
-
The Future Is Noninvasive: A Brief Review of the Evolution and Clinical Utility of Vagus Nerve Stimulation.Focus (Am Psychiatr Publ). 2022 Jan;20(1):3-7. doi: 10.1176/appi.focus.20210023. Epub 2022 Jan 25. Focus (Am Psychiatr Publ). 2022. PMID: 35746934 Free PMC article. Review.
Cited by
-
Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis.J Clin Med. 2023 May 25;12(11):3673. doi: 10.3390/jcm12113673. J Clin Med. 2023. PMID: 37297867 Free PMC article. Review.
-
Future horizons in diabetes: integrating AI and personalized care.Front Endocrinol (Lausanne). 2025 Mar 27;16:1583227. doi: 10.3389/fendo.2025.1583227. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40213102 Free PMC article. Review.
-
State of the art: non-invasive electrical stimulation for the treatment of chronic tinnitus.Ther Adv Chronic Dis. 2023 Jan 18;14:20406223221148061. doi: 10.1177/20406223221148061. eCollection 2023. Ther Adv Chronic Dis. 2023. PMID: 36860934 Free PMC article. Review.
-
Direct and Transcutaneous Vagus Nerve Stimulation for Treatment of Tinnitus: A Scoping Review.Front Neurosci. 2021 May 28;15:680590. doi: 10.3389/fnins.2021.680590. eCollection 2021. Front Neurosci. 2021. PMID: 34122002 Free PMC article.
-
Transcutaneous auricular vagus nerve stimulation for the treatment of myoarthropatic symptoms in patients with craniomandibular dysfunction - a protocol for a randomized and controlled pilot trial.Pilot Feasibility Stud. 2024 Feb 8;10(1):27. doi: 10.1186/s40814-024-01447-x. Pilot Feasibility Stud. 2024. PMID: 38331976 Free PMC article.
References
-
- Antonino D., Teixeira A. L., Maia-Lopes P. M., Souza M. C., Sabino-Carvalho J. L., Murray A. R., et al. (2017). Non-invasive vagus nerve stimulation acutely improves spontaneous cardiac baroreflex sensitivity in healthy young men: a randomized placebo-controlled trial. Brain Stimul. 10 875–881. 10.1016/j.brs.2017.05.006 - DOI - PubMed
-
- Aviles R. J., Martin D. O., Apperson-Hansen C., Houghtaling P. L., Rautaharju P., Kronmal R. A., et al. (2003). Inflammation as a risk factor for atrial fibrillation. Circulation 108 3006–3010. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials