

Audiovestibular Quantification in Rare Third Window Disorders in Children
- PMID: 33041966
- PMCID: PMC7526203
- DOI: 10.3389/fneur.2020.00954
Audiovestibular Quantification in Rare Third Window Disorders in Children
Abstract
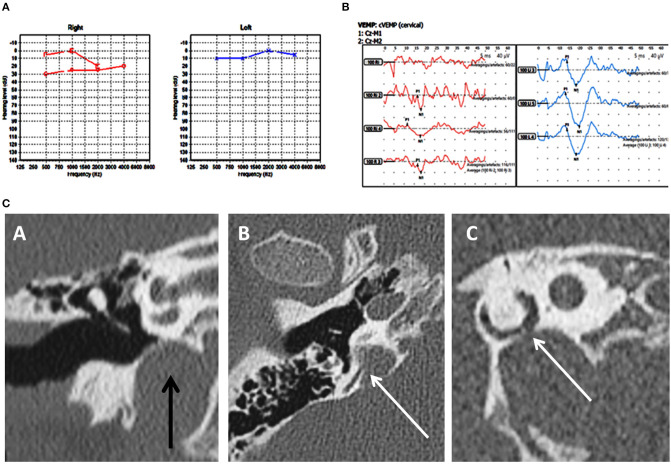
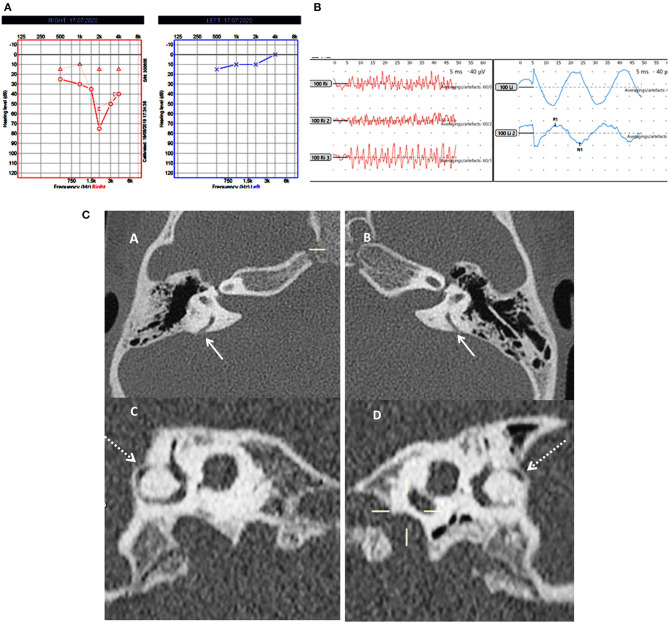
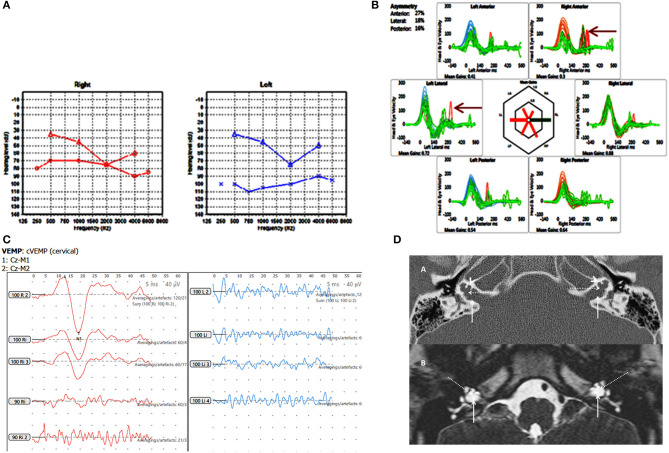
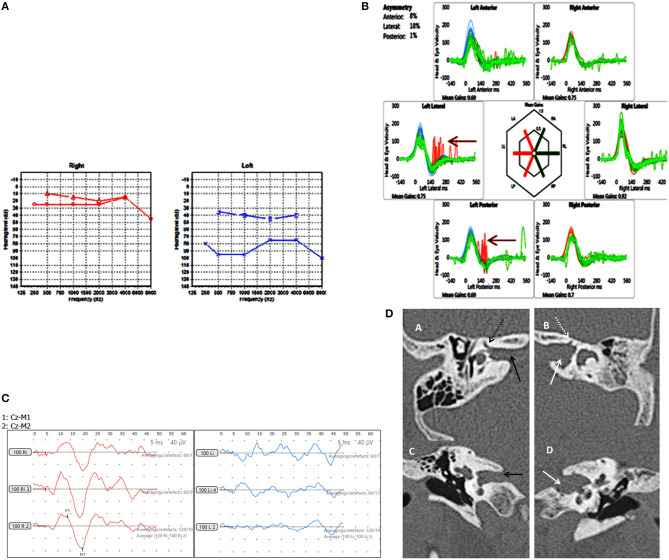
Third window disorders are structural abnormalities in the bony otic capsule that establish a connection between the middle/inner ear or the inner ear/cranial cavity. Investigated extensively in adults, they have hardly been studied in children. This study is a retrospective study of children (aged 5-17 years) diagnosed with rare third window disorders (third window disorders reported rarely or not reported in children) in a tertiary pediatric vestibular unit in the United Kingdom. It aimed to investigate audiovestibular function in these children. Final diagnosis was achieved by high resolution CT scan of the temporal bones. Of 920 children attending for audiovestibular assessment over a 42 month period, rare third windows were observed in 8 (<1%). These included posterior semicircular canal dehiscence (n = 3, 0.3%), posterior semicircular canal thinning (n = 2, 0.2%), X linked gusher (n = 2, 0.2%), and a combination of dilated internal auditory meatus/irregular cochlear partition/deficient facial nerve canal (n = 1, 0.1%). The majority of them (87.5%) demonstrated a mixed/conductive hearing loss with an air-bone gap in the presence of normal tympanometry (100%). Transient otoacoustic emissions were absent with a simultaneous cochlear pathology in 50% of the cohort. Features of disequilibrium were observed in 75% and about a third showed deranged vestibular function tests. Video head impulse test abnormalities were detected in 50% localizing to the side of the lesion. Cervical vestibular evoked myogenic potential test abnormalities were observed in all children in the cohort undergoing the test where low thresholds and high amplitudes classically found in third window disorders localized to the side of the defects in 28.5%. In the series, 71.4% also demonstrated absent responses/amplitude asymmetry, some of which did not localize to the ipsilesional side. Two children presented with typical third window symptoms. This study observes 2 new rare pediatric third window phenotypes and the presence of a cochlear hearing loss in these disorders. It emphasizes that these disorders should be considered as an etiology of hearing loss/disequilibrium in children. It also suggests that pediatric third window disorders may not present with classical third window features and are variable in their presentations/audiovestibular functions.
Keywords: HRCT; X linked gusher; audiovestibular; cVEMP; children; semicircular canal dehiscence; third window; vHIT.
Copyright © 2020 Dasgupta, Ratnayake, Crunkhorn, Iqbal, Strachan and Avula.
Figures
Similar articles
-
X-Linked Gusher Disease DFNX2 in Children, a Rare Inner Ear Dysplasia with Mixed Hearing and Vestibular Loss.Audiol Res. 2023 Aug 4;13(4):600-614. doi: 10.3390/audiolres13040052. Audiol Res. 2023. PMID: 37622928 Free PMC article.
-
Functional and Objective Audiovestibular Evaluation of Children With Apparent Semicircular Canal Dehiscence-A Case Series in a Pediatric Vestibular Center.Front Neurol. 2019 Apr 2;10:306. doi: 10.3389/fneur.2019.00306. eCollection 2019. Front Neurol. 2019. PMID: 31001191 Free PMC article.
-
Conductive hearing loss caused by third-window lesions of the inner ear.Otol Neurotol. 2008 Apr;29(3):282-9. doi: 10.1097/mao.0b013e318161ab24. Otol Neurotol. 2008. PMID: 18223508 Free PMC article. Review.
-
Posterior semicircular canal dehiscence: first reported case series.Otol Neurotol. 2010 Feb;31(2):339-44. doi: 10.1097/MAO.0b013e3181be65a4. Otol Neurotol. 2010. PMID: 19841602
-
Spectrum of Third Window Abnormalities: Semicircular Canal Dehiscence and Beyond.AJNR Am J Neuroradiol. 2017 Jan;38(1):2-9. doi: 10.3174/ajnr.A4922. Epub 2016 Aug 25. AJNR Am J Neuroradiol. 2017. PMID: 27561833 Free PMC article. Review.
Cited by
-
X-Linked Gusher Disease DFNX2 in Children, a Rare Inner Ear Dysplasia with Mixed Hearing and Vestibular Loss.Audiol Res. 2023 Aug 4;13(4):600-614. doi: 10.3390/audiolres13040052. Audiol Res. 2023. PMID: 37622928 Free PMC article.
-
Posterior Semicircular Canal Dehiscence with Vestibulo-Ocular Reflex Reduction for the Affected Canal at the Video-Head Impulse Test: Considerations to Pathomechanisms.Audiol Res. 2024 Mar 24;14(2):317-332. doi: 10.3390/audiolres14020028. Audiol Res. 2024. PMID: 38666899 Free PMC article.
-
Audio-Vestibular Evaluation of Pediatric Pseudo-Conductive Hearing Loss: Third Window Syndromes.Audiol Res. 2024 Sep 6;14(5):790-798. doi: 10.3390/audiolres14050066. Audiol Res. 2024. PMID: 39311219 Free PMC article. Review.
-
The Third Mobile Window Syndrome: A Clinical Spectrum of Different Anatomical Locations-Characterization, Therapeutic Response, and Implications in the Development of Endolymphatic Hydrops.J Clin Med. 2024 Nov 28;13(23):7232. doi: 10.3390/jcm13237232. J Clin Med. 2024. PMID: 39685691 Free PMC article.
-
Clinical Profile, Trends, and Management in Pediatric Patients with Audiovestibular Disorders: Can We Predict Emotional Disability in Pediatric Patients with Episodes of Vertigo and Dizziness?Audiol Res. 2024 Aug 14;14(4):701-713. doi: 10.3390/audiolres14040059. Audiol Res. 2024. PMID: 39194415 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous