

Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment
- PMID: 33041986
- PMCID: PMC7522398
- DOI: 10.3389/fneur.2020.01046
Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment
Abstract
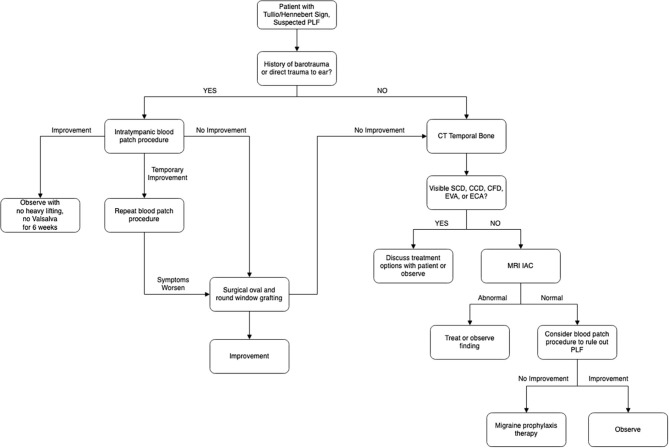
A perilymphatic fistula (PLF) is an abnormal communication between the perilymph-filled inner ear and the middle ear cavity, mastoid, or intracranial cavity. A PLF most commonly forms when the integrity of the oval or round window is compromised, and it may be trauma-induced or may occur with no known cause (idiopathic). Controversy regarding the diagnosis of idiopathic PLF has persisted for decades, and the presenting symptoms may be vague. However, potential exists for this condition to be one of the few etiologies of dizziness, tinnitus, and hearing loss that can be treated surgically. The aim of this review is to provide an update on classification, diagnosis, and treatment of PLF. Particular attention will be paid to idiopathic PLF and conditions that may have a similar presentation, with subsequent information on how best to distinguish them. Novel diagnostic criteria for PLF and management strategy for PLF and PLF-like symptoms is presented.
Keywords: association; blood patch; dizziness; perilymph fistula; perilymphatic fistula; tinnitus; vertigo.
Copyright © 2020 Sarna, Abouzari, Merna, Jamshidi, Saber and Djalilian.
Figures

References
-
- E. R. Fistel im ovalen Fenester. Monatsschr Ohrenh. (1909) 10:787.
-
- Friedland DR, Wackym PA. A critical appraisal of spontaneous perilymphatic fistulas of the inner ear. Am J Otol. (1999) 20:261–76. - PubMed