

Development and Interpretation of Multiple Machine Learning Models for Predicting Postoperative Delayed Remission of Acromegaly Patients During Long-Term Follow-Up
- PMID: 33042013
- PMCID: PMC7525125
- DOI: 10.3389/fendo.2020.00643
Development and Interpretation of Multiple Machine Learning Models for Predicting Postoperative Delayed Remission of Acromegaly Patients During Long-Term Follow-Up
Abstract
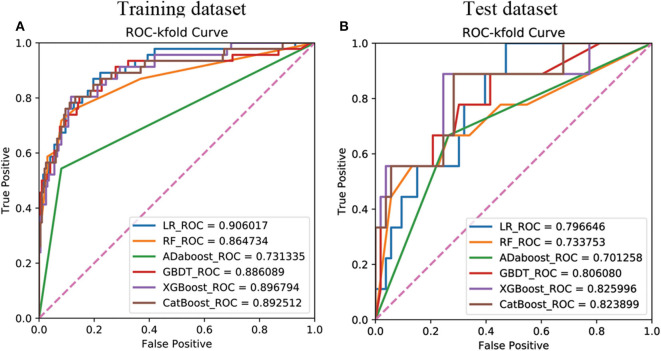
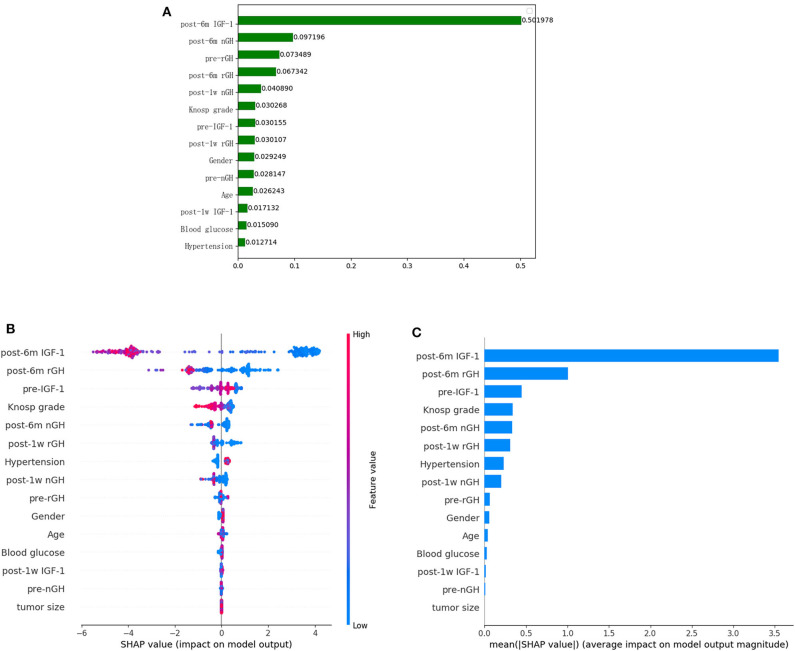
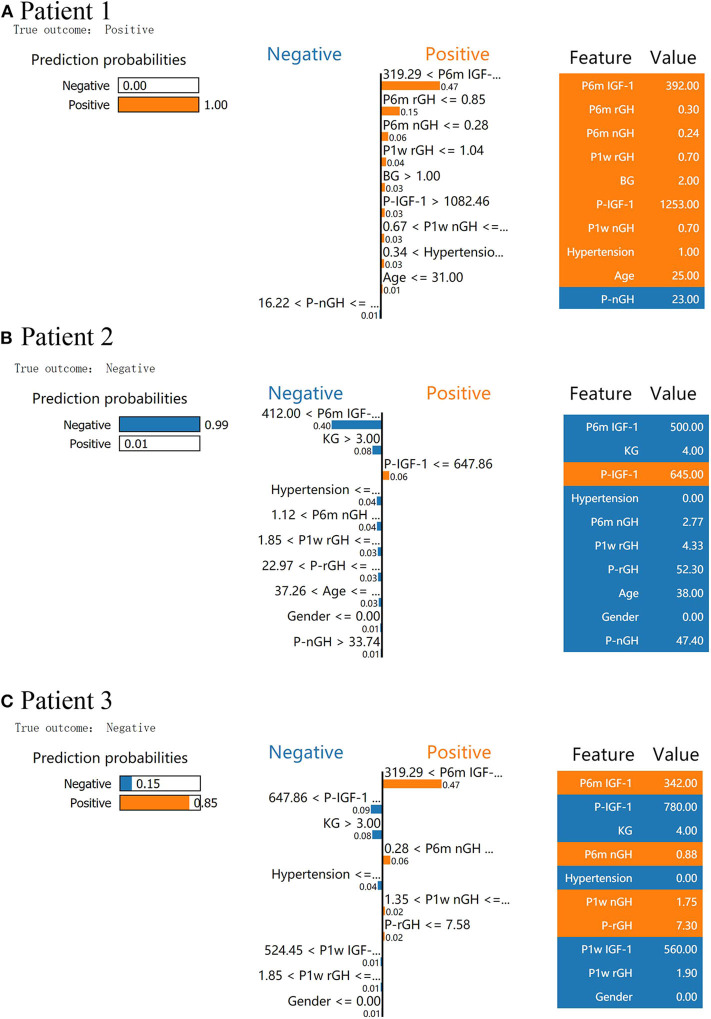
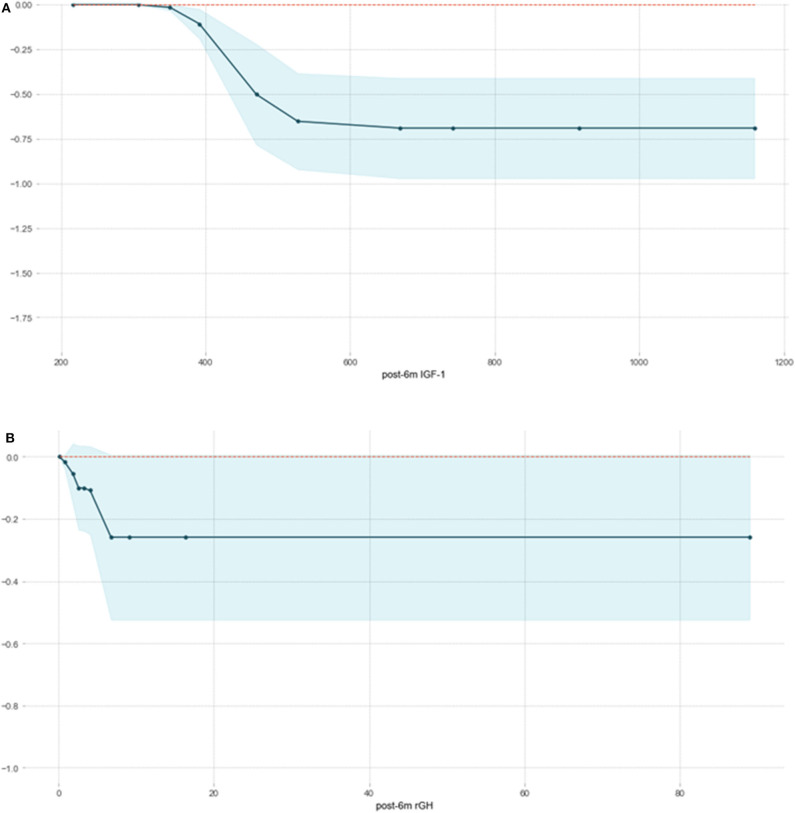
Background: Some patients with acromegaly do not reach the remission standard in the short term after surgery but achieve remission without additional postoperative treatment during long-term follow-up; this phenomenon is defined as postoperative delayed remission (DR). DR may complicate the interpretation of surgical outcomes in patients with acromegaly and interfere with decision-making regarding postoperative adjuvant therapy. Objective: We aimed to develop and validate machine learning (ML) models for predicting DR in acromegaly patients who have not achieved remission within 6 months of surgery. Methods: We enrolled 306 acromegaly patients and randomly divided them into training and test datasets. We used the recursive feature elimination (RFE) algorithm to select features and applied six ML algorithms to construct DR prediction models. The performance of these ML models was validated using receiver operating characteristics analysis. We used permutation importance, SHapley Additive exPlanations (SHAP), and local interpretable model-agnostic explanation (LIME) algorithms to determine the importance of the selected features and interpret the ML models. Results: Fifty-five (17.97%) acromegaly patients met the criteria for DR, and five features (post-1w rGH, post-1w nGH, post-6m rGH, post-6m IGF-1, and post-6m nGH) were significantly associated with DR in both the training and the test datasets. After the RFE feature selection, the XGboost model, which comprised the 15 important features, had the greatest discriminatory ability (area under the curve = 0.8349, sensitivity = 0.8889, Youden's index = 0.6842). The XGboost model showed good discrimination ability and provided significantly better estimates of DR of patients with acromegaly compared with using only the Knosp grade. The results obtained from permutation importance, SHAP, and LIME algorithms showed that post-6m IGF-1 is the most important feature in XGboost algorithm prediction and showed the reliability and the clinical practicability of the XGboost model in DR prediction. Conclusions: ML-based models can serve as an effective non-invasive approach to predicting DR and could aid in determining individual treatment and follow-up strategies for acromegaly patients who have not achieved remission within 6 months of surgery.
Keywords: LIME; SHAP; acromegaly; delayed remission; machine learning.
Copyright © 2020 Dai, Fan, Li, Bao, Li, Su, Yao, Deng, Xing, Feng, Feng and Wang.
Figures
Similar articles
-
Development of Machine Learning Models for Predicting Postoperative Delayed Remission in Patients With Cushing's Disease.J Clin Endocrinol Metab. 2021 Jan 1;106(1):e217-e231. doi: 10.1210/clinem/dgaa698. J Clin Endocrinol Metab. 2021. PMID: 33000120
-
Development and assessment of machine learning algorithms for predicting remission after transsphenoidal surgery among patients with acromegaly.Endocrine. 2020 Feb;67(2):412-422. doi: 10.1007/s12020-019-02121-6. Epub 2019 Oct 30. Endocrine. 2020. PMID: 31673954
-
Machine learning-enabled prediction of prolonged length of stay in hospital after surgery for tuberculosis spondylitis patients with unbalanced data: a novel approach using explainable artificial intelligence (XAI).Eur J Med Res. 2024 Jul 25;29(1):383. doi: 10.1186/s40001-024-01988-0. Eur J Med Res. 2024. PMID: 39054495 Free PMC article.
-
Evolving criteria for post-operative biochemical remission of acromegaly: can we achieve a definitive cure? An audit of surgical results on a large series and a review of the literature.Endocr Relat Cancer. 2003 Dec;10(4):611-9. doi: 10.1677/erc.0.0100611. Endocr Relat Cancer. 2003. PMID: 14713271 Review.
-
Treatment of acromegaly by endoscopic transsphenoidal surgery: surgical experience in 214 cases and cure rates according to current consensus criteria.J Neurosurg. 2013 Dec;119(6):1467-77. doi: 10.3171/2013.8.JNS13224. Epub 2013 Sep 27. J Neurosurg. 2013. PMID: 24074496 Review.
Cited by
-
Diagnosis of Cushing's syndrome with generalized linear model and development of mobile application.Medicine (Baltimore). 2025 Jun 20;104(25):e42910. doi: 10.1097/MD.0000000000042910. Medicine (Baltimore). 2025. PMID: 40550094 Free PMC article.
-
Predictive models for endoscopic disease activity in patients with ulcerative colitis: Practical machine learning-based modeling and interpretation.Front Med (Lausanne). 2022 Dec 21;9:1043412. doi: 10.3389/fmed.2022.1043412. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36619650 Free PMC article.
-
Development and validation of an explainable machine learning model for predicting multidimensional frailty in hospitalized patients with cirrhosis.Brief Bioinform. 2024 Sep 23;25(6):bbae491. doi: 10.1093/bib/bbae491. Brief Bioinform. 2024. PMID: 39358034 Free PMC article.
-
The Application of Artificial Intelligence and Machine Learning in Pituitary Adenomas.Front Oncol. 2021 Dec 23;11:784819. doi: 10.3389/fonc.2021.784819. eCollection 2021. Front Oncol. 2021. PMID: 35004306 Free PMC article. Review.
-
Machine Learning Models for Predicting In-Hospital Mortality in Acute Aortic Dissection Patients.Front Cardiovasc Med. 2021 Sep 17;8:727773. doi: 10.3389/fcvm.2021.727773. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34604356 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous