

Association Between Vitamin D Status and Diabetic Complications in Patients With Type 2 Diabetes Mellitus: A Cross-Sectional Study in Hunan China
- PMID: 33042022
- PMCID: PMC7525149
- DOI: 10.3389/fendo.2020.564738
Association Between Vitamin D Status and Diabetic Complications in Patients With Type 2 Diabetes Mellitus: A Cross-Sectional Study in Hunan China
Abstract
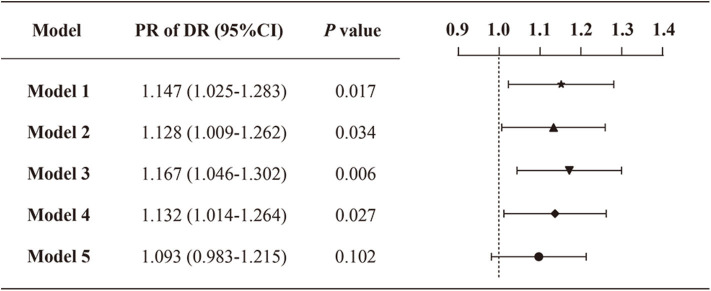
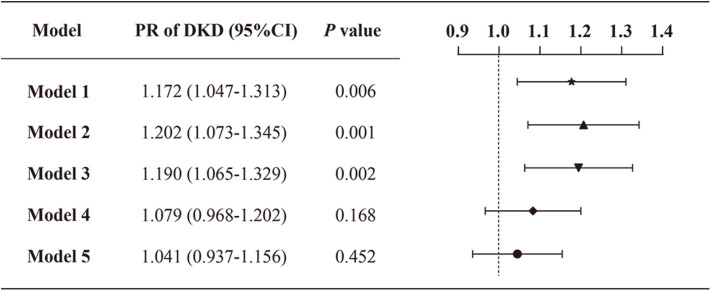
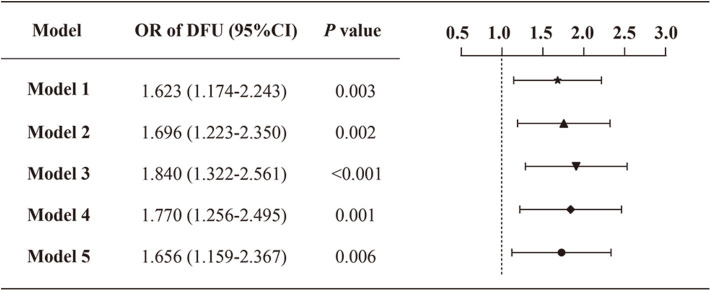
Background: Vitamin D status has been linked to diabetes-related complications due to multiple extraskeletal effects. We aimed to investigate the association between vitamin D deficiency (VDD) and diabetic vascular complications, including diabetic retinopathy (DR), diabetic kidney disease (DKD), and diabetic foot ulcers (DFU). Methods: A total of 4,284 Chinese patients with type 2 diabetic mellitus (T2DM) were enrolled into the cross-sectional study. VDD was defined as serum 25-hydroxyvitamin D <50 nmol/L. Demographic data, physical measurements, laboratory measurements, comorbidities, and related medications were collected and analyzed by VDD status. Poisson regression with robust variance estimation and binary logistic regression were performed to explore the relationship between VDD and diabetic complications. Results: The prevalence of VDD, DR, DKD, DFU accounted to 71.7% (95% confidence intervals [CI]: 70.3-73.0%), 28.5% (95% CI: 27.2-29.9%), 28.2% (95% CI: 26.8-29.5%), and 5.7% (95% CI: 5.1-6.5%), respectively. The prevalence ratios (95% CI) for DR and DKD by VDD status, adjusted for demographics, physical measurements, laboratory measurements, related complications, and comorbidities, and medications, were 1.093 (0.983-1.215) and 1.041 (0.937-1.156), respectively. The odds ratio (95% CI) for DFU by VDD status was 1.656 (1.159-2.367) in the final adjusted model. Meanwhile, the prevalence of VDD was significantly higher in patients with DFU compared with patients without DFU. Conclusions: The present study firstly indicated that VDD was significantly associated with a higher prevalence of DFU among Chinese T2DM patients. The association between VDD status and DR or DKD was not significant when adjusting for all potential covariates. Vitamin D screening or supplementation may be beneficial to prevent DFU and improve the prognosis of T2DM patients.
Keywords: cross-sectional study; diabetic foot ulcers; diabetic kidney disease; diabetic retinopathy; vitamin D deficiency.
Copyright © 2020 Xiao, Wei, Xiong, Yang and Sun.
Figures
Similar articles
-
Risk of Insufficient Hydroxyvitamin D Levels in Diabetic Foot Ulcers in Rivers State Nigeria.West Afr J Med. 2025 Mar 31;42(3):225-230. West Afr J Med. 2025. PMID: 40845204
-
Association of serum vitamin D levels and diabetic retinopathy in Asian Indians with type 2 diabetes.Diabetes Res Clin Pract. 2018 May;139:308-313. doi: 10.1016/j.diabres.2018.02.040. Epub 2018 Mar 5. Diabetes Res Clin Pract. 2018. PMID: 29518485
-
Raised serum 25-hydroxyvitamin D levels in patients with active diabetic foot ulcers.Br J Nutr. 2016 Jun;115(11):1938-46. doi: 10.1017/S0007114516001094. Br J Nutr. 2016. PMID: 27153203
-
Vitamin D and diabetic foot ulcer: a systematic review and meta-analysis.Nutr Diabetes. 2019 Mar 11;9(1):8. doi: 10.1038/s41387-019-0078-9. Nutr Diabetes. 2019. PMID: 30858355 Free PMC article.
-
Vitamin D deficiency and its associated factors among patients with type 2 diabetes mellitus: a systematic review and meta-analysis.BMJ Open. 2023 Oct 5;13(10):e075607. doi: 10.1136/bmjopen-2023-075607. BMJ Open. 2023. PMID: 37798019 Free PMC article.
Cited by
-
The correlation between serum vitamin D status and the occurrence of diabetic foot ulcers: a comprehensive systematic review and meta-analysis.Sci Rep. 2024 Sep 20;14(1):21932. doi: 10.1038/s41598-024-73133-0. Sci Rep. 2024. PMID: 39304728 Free PMC article.
-
Level of 25-hydroxyvitamin D and vitamin D receptor in diabetic foot ulcer and factor associated with diabetic foot ulcers.Diabetol Metab Syndr. 2023 Feb 24;15(1):30. doi: 10.1186/s13098-023-01002-3. Diabetol Metab Syndr. 2023. PMID: 36829206 Free PMC article.
-
Serum 25-Hydroxyvitamin D Level Is Positively Associated with Vascular Reactivity Index in Patients with Type 2 Diabetes Mellitus.Nutrients. 2024 May 23;16(11):1575. doi: 10.3390/nu16111575. Nutrients. 2024. PMID: 38892508 Free PMC article.
-
Clinical, metabolic, and immunological characterisation of adult Ugandan patients with new-onset diabetes and low vitamin D status.BMC Endocr Disord. 2022 Sep 15;22(1):230. doi: 10.1186/s12902-022-01148-7. BMC Endocr Disord. 2022. PMID: 36109715 Free PMC article.
-
The Role of Vitamin D in Diabetic Nephropathy: A Translational Approach.Int J Mol Sci. 2022 Jan 12;23(2):807. doi: 10.3390/ijms23020807. Int J Mol Sci. 2022. PMID: 35054991 Free PMC article. Review.
References
-
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. . Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract. (2019) 157:107843. 10.1016/j.diabres.2019.107843 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical