

Clinical Radiobiology of Fast Neutron Therapy: What Was Learnt?
- PMID: 33042798
- PMCID: PMC7522468
- DOI: 10.3389/fonc.2020.01537
Clinical Radiobiology of Fast Neutron Therapy: What Was Learnt?
Abstract
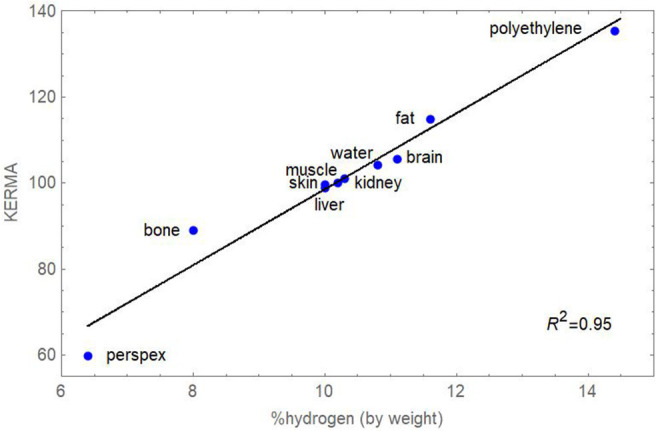
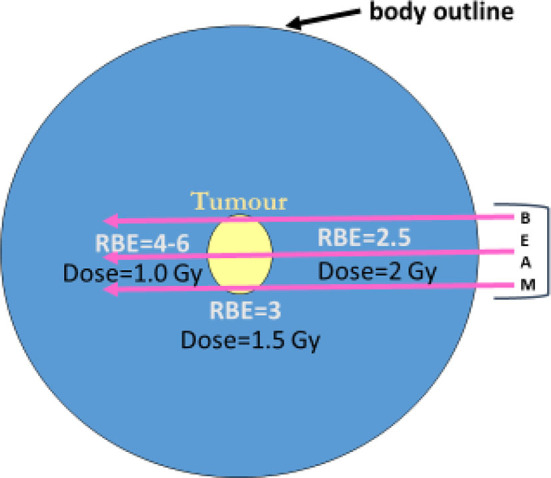
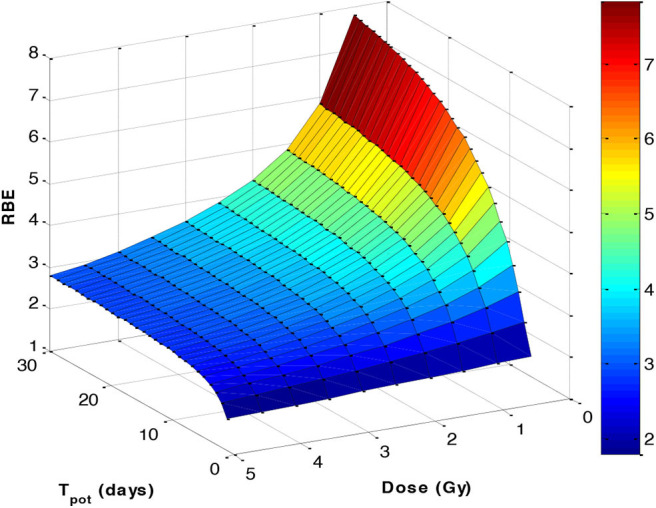
Neutron therapy was developed from neutron radiobiology experiments, and had identified a higher cell kill per unit dose and an accompanying reduction in oxygen dependency. But experts such as Hal Gray were sceptical about clinical applications, for good reasons. Gray knew that the increase in relative biological effectiveness (RBE) with dose fall-off could produce marked clinical limitations. After many years of research, this treatment did not produce the expected gains in tumour control relative to normal tissue toxicity, as predicted by Gray. More detailed reasons for this are discussed in this paper. Neutrons do not have Bragg peaks and so did not selectively spare many tissues from radiation exposure; the constant neutron RBE tumour prescription values did not represent the probable higher RBE values in late-reacting tissues with low α/β values; the inevitable increase in RBE as dose falls along a beam would also contribute to greater toxicity than in a similar megavoltage photon beam. Some tissues such as the central nervous system white matter had the highest RBEs partly because of the higher percentage hydrogen content in lipid-containing molecules. All the above factors contributed to disappointing clinical results found in a series of randomised controlled studies at many treatment centres, although at the time they were performed, neutron therapy was in a catch-up phase with photon-based treatments. Their findings are summarised along with their technical aspects and fractionation choices. Better understanding of fast neutron experiments and therapy has been gained through relatively simple mathematical models-using the biological effective dose concept and incorporating the RBEmax and RBEmin parameters (the limits of RBE at low and high dose, respectively-as shown in the Appendix). The RBE itself can then vary between these limits according to the dose per fraction used. These approaches provide useful insights into the problems that can occur in proton and ion beam therapy and how they may be optimised. This is because neutron ionisations in living tissues are mainly caused by recoil protons of energy proportional to the neutron energy: these are close to the proton energies that occur close to the Bragg peak region. To some extent, neutron RBE studies contain the highest RBE ranges found within proton and ion beams near Bragg peaks. In retrospect, neutrons were a useful radiobiological tool that has continued to inform the scientific and clinical community about the essential radiobiological principles of all forms of high linear energy transfer therapy. Neutron radiobiology and its implications should be taught on training courses and studied closely by clinicians, physicists, and biologists engaged in particle beam therapies.
Keywords: RBE; hadron; high LET; neutron therapy; radiobiology; radiotherapy.
Copyright © 2020 Jones.
Figures
Similar articles
-
Radiobiology with heavy charged particles: a historical review.Phys Med. 1998 Jul;14 Suppl 1:1-19. Phys Med. 1998. PMID: 11542635
-
Fast neutron energy based modelling of biological effectiveness with implications for proton and ion beams.Phys Med Biol. 2021 Feb 14;66(4):045028. doi: 10.1088/1361-6560/abddd0. Phys Med Biol. 2021. PMID: 33472183
-
Intestinal crypt regeneration in mice: a biological system for quality assurance in non-conventional radiation therapy.Radiother Oncol. 2004 Dec;73 Suppl 2:S148-54. doi: 10.1016/s0167-8140(04)80038-0. Radiother Oncol. 2004. PMID: 15971332
-
Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer.Phys Med Biol. 2014 Nov 21;59(22):R419-72. doi: 10.1088/0031-9155/59/22/R419. Epub 2014 Oct 31. Phys Med Biol. 2014. PMID: 25361443 Review.
-
The radiobiological principles of boron neutron capture therapy: a critical review.Appl Radiat Isot. 2011 Dec;69(12):1756-9. doi: 10.1016/j.apradiso.2011.04.019. Epub 2011 Apr 22. Appl Radiat Isot. 2011. PMID: 21543233 Review.
Cited by
-
Fast and Furious: Fast Neutron Therapy in Cancer Treatment.Int J Part Ther. 2022 Aug 5;9(2):59-69. doi: 10.14338/IJPT-22-00017. eCollection 2022 Fall. Int J Part Ther. 2022. PMID: 36060415 Free PMC article. Review.
-
Growth hormone and radiation therapy: friend, foe, or both?Endocr Relat Cancer. 2024 Jan 24;31(3):e220371. doi: 10.1530/ERC-22-0371. Print 2024 Mar 1. Endocr Relat Cancer. 2024. PMID: 38174978 Free PMC article. Review.
-
Adenoid cystic carcinoma: insights from molecular characterization and therapeutic advances.MedComm (2020). 2024 Sep 11;5(9):e734. doi: 10.1002/mco2.734. eCollection 2024 Sep. MedComm (2020). 2024. PMID: 39263605 Free PMC article. Review.
-
An Evaluation of the Potential Radiosensitization Effect of Spherical Gold Nanoparticles to Induce Cellular Damage Using Different Radiation Qualities.Molecules. 2025 Feb 24;30(5):1038. doi: 10.3390/molecules30051038. Molecules. 2025. PMID: 40076263 Free PMC article.
-
Treatment of a Non-syndromic Carotid Body Paraganglioma Using Fast Neutron Radiotherapy: A Case Report and Review of Literature.Cureus. 2023 Sep 4;15(9):e44673. doi: 10.7759/cureus.44673. eCollection 2023 Sep. Cureus. 2023. PMID: 37799247 Free PMC article.
References
-
- Fowler JF. Chapter 4. Types of radiation and their sources. Medical physics handbooks. In: Nucelar Particles in Cancer Treatment. Bristol: Adam Hilger; (1981).
-
- Nutting CM, Morden JP, Harrington KJ, Urbano TG, Bhide SA, Clark C, et al. . Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol. (2011) 12:127–36 10.1016/S1470-2045(10)70290-4 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources