

Circulating Tumor DNA as a Prognostic Biomarker in Localized Non-small Cell Lung Cancer
- PMID: 33042842
- PMCID: PMC7523087
- DOI: 10.3389/fonc.2020.561598
Circulating Tumor DNA as a Prognostic Biomarker in Localized Non-small Cell Lung Cancer
Abstract
Background: Routine clinical surveillance involves serial radiographic imaging following radical surgery in localized non-small cell lung cancer (NSCLC). However, such surveillance can detect only macroscopic disease recurrence and is frequently inconclusive. We investigated if detection of ctDNA before and after resection of NSCLC identifies the patients with risk of relapse, and furthermore, informs about response to management.
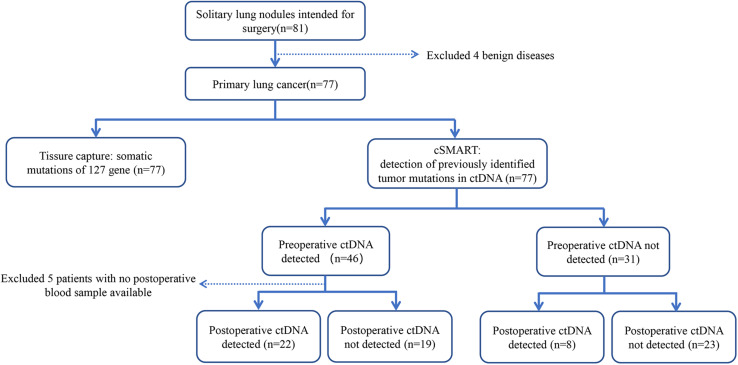
Methods: We recruited a total of 77 NSCLC patients. A high-throughput 127 target-gene capture technology and a high-sensitivity circulating single-molecule amplification and resequencing technology (cSMART) assay were used to detect the somatic mutations in the tumor tissues as well as the plasma of NSCLC patients before and after surgery to monitor for minimal residual disease (MRD). Kaplan-Meier and Cox regression analysis were performed to evaluate the relapse-free survival (RFS) and overall survival (OS) of patients with predictor variables.
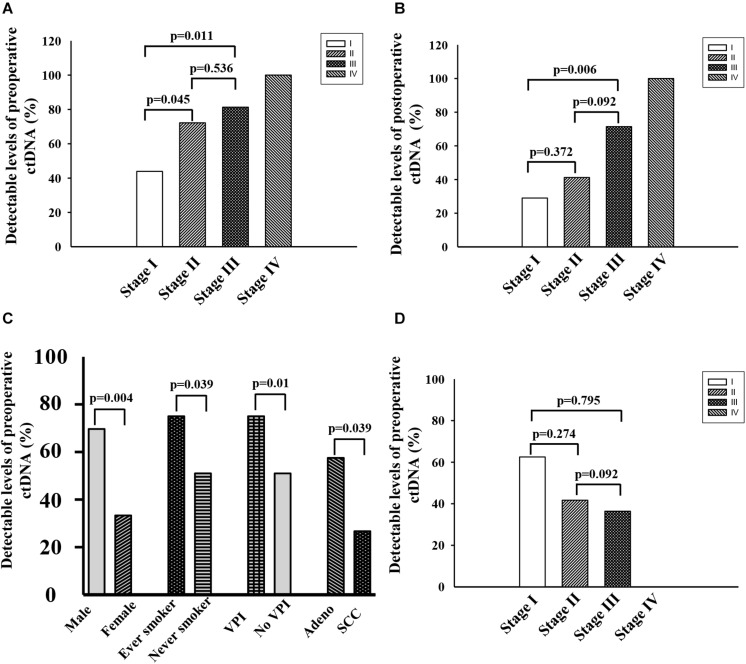
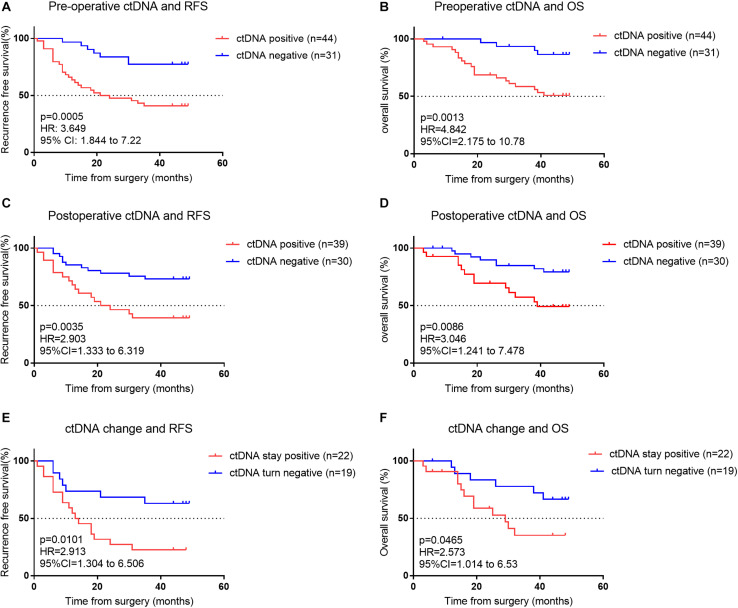
Results: Patients with a higher stage (III/IV) and preoperative ctDNA-positive status demonstrated a significant 2.8-3.4-fold risk and 3.8-4.0-fold risk for recurrence and death, respectively. Preoperative ctDNA-positive patients associated with a lower RFS (HR = 3.812, p = 0.0005) and OS (HR = 5.004, p = 0.0009). Postoperative ctDNA-positive patients also associated with a lower RFS (HR = 3.076, p = 0.0015) and OS (HR = 3.195, p = 0.0053). Disease recurrence occurred among 63.3% (19/30) of postoperative ctDNA-positive patients. Most of these patients 89.5% (17/19) had detectable ctDNA within 2 weeks after surgery and was identified in advance of radiographic findings by a median of 12.6 months.
Conclusion: Advanced stage and preoperative ctDNA-positive are strong predictors of RFS and OS in localized NSCLC patients undergoing complete resection. Postoperative detection of ctDNA increases chance to detect early relapse, thus can fulfill an important role in stratifying patients for immediate further treatment with adjuvant and neoadjuvant therapy.
Keywords: circulating single molecule amplification and re-sequencing technology; circulating tumor DNA; minimal residual disease; non-small cell lung cancer; prognostic biomarker.
Copyright © 2020 Peng, Huang, Yin, Tan, Chen, Liu, Tang, Wang, Zhang, Zou, Li, Su, Wang, Chin and Yu.
Figures
References
LinkOut - more resources
Full Text Sources