

Management of Children With Fever at Risk for Pediatric Sepsis: A Prospective Study in Pediatric Emergency Care
- PMID: 33042929
- PMCID: PMC7527403
- DOI: 10.3389/fped.2020.548154
Management of Children With Fever at Risk for Pediatric Sepsis: A Prospective Study in Pediatric Emergency Care
Abstract
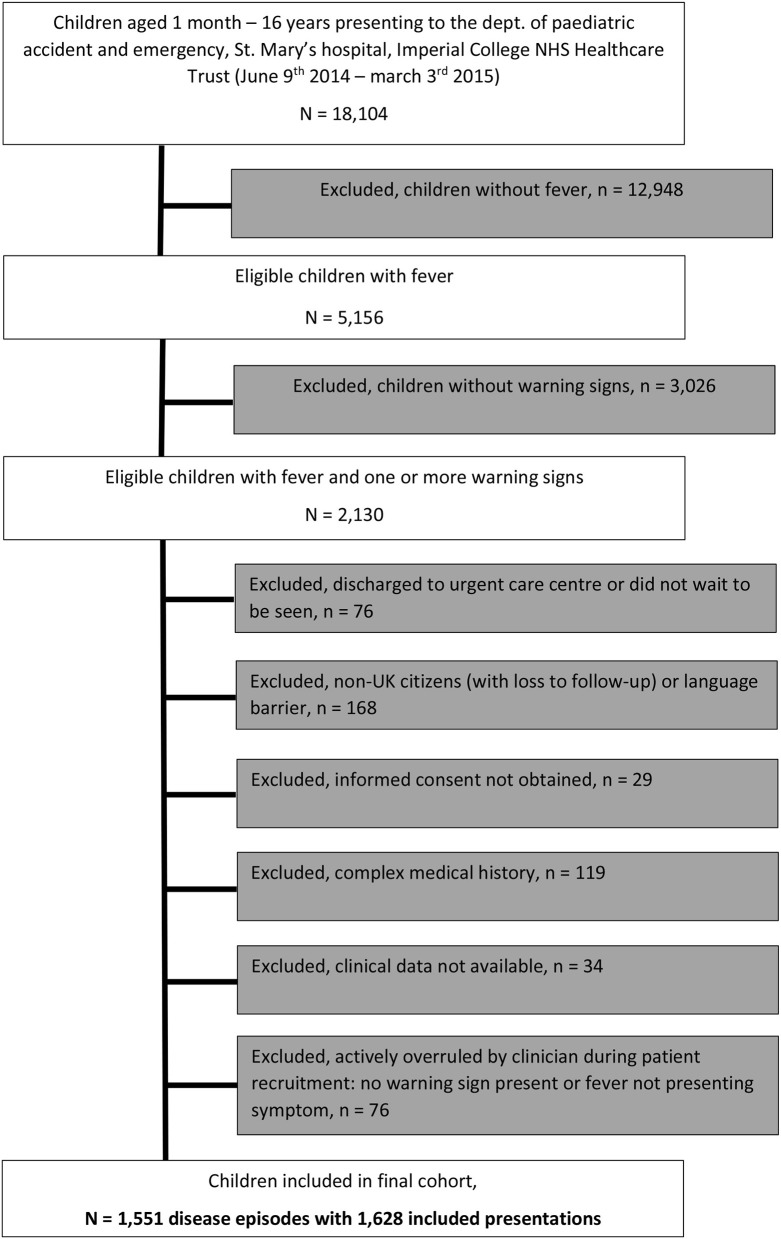
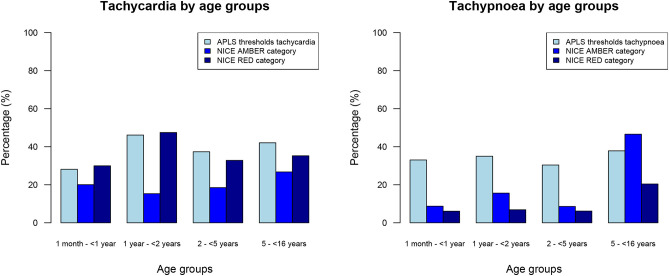
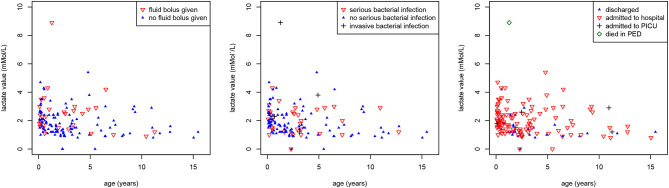
Objective: To study warning signs of serious infections in febrile children presenting to PED, ascertain their risk of having sepsis, and evaluate their management. Design: Prospective observational study. Setting: A single pediatric emergency department (PED). Participants: Febrile children, aged 1 month-16 years, with >= 1 warning signs of sepsis. Interventions and Main outcome measures: Clinical characteristics, including different thresholds for tachycardia and tachypnoea, and their association with (1) delivery of pediatric sepsis 6 (PS6) interventions, (2) final diagnosis of invasive bacterial infection (IBI), (3) the risk for pediatric intensive care unit (PICU) admission, and (4) death. Results: Forty-one percent of 5,156 febrile children had warning signs of sepsis. 1,606 (34%) children had tachypnoea and 1,907 (39%) children had tachycardia when using APLS threshold values. Using the NICE sepsis guidelines thresholds resulted in 1,512 (32%) children having tachypnoea (kappa 0.56) and 2,769 (57%) children having tachycardia (kappa 0.66). Of 1,628 PED visits spanning 1,551 disease episodes, six children (0.4%) had IBI, with one death (0.06%), corresponding with 256 children requiring escalation of care according to sepsis guideline recommendations for each child with IBI. There were five additional PICU admissions (0.4%). 121 (7%) had intravenous antibiotics in PED; 39 children (2%) had an intravenous fluid bolus, inotrope drugs were started in one child. 440 children (27%) were reviewed by a senior clinician. In 4/11 children with IBI or PICU admission or death, PS6 interventions were delivered within 60 min after arriving. 1,062 (65%) visits had no PS6 interventions. Diagnostic performance of vital signs or sepsis criteria for predicting serious illness yielded a large proportion of false positives. Lactataemia was not associated with giving iv fluid boluses (p = 0.19) or presence of serious bacterial infections (p = 0.128). Conclusion: Many febrile children (41%) present with warning signs for sepsis, with only few of them undergoing investigations or treatment for true sepsis. Children with positive isolates in blood or CSF culture presented in a heterogeneous manner, with varying levels of urgency and severity of illness. Delivery of sepsis care can be improved in only a minority of children with IBI or admitted to PICU.
Keywords: child; clinical tools; fever; pediatric sepsis interventions; sepsis.
Copyright © 2020 Nijman, Jorgensen, Levin, Herberg and Maconochie.
Figures
References
-
- Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, et al. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ. (2010) 340:1015. 10.1136/bmj.c1594 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources