

Phenotypic characterisation of early COPD: a prospective case-control study
- PMID: 33043045
- PMCID: PMC7533304
- DOI: 10.1183/23120541.00047-2020
Phenotypic characterisation of early COPD: a prospective case-control study
Abstract
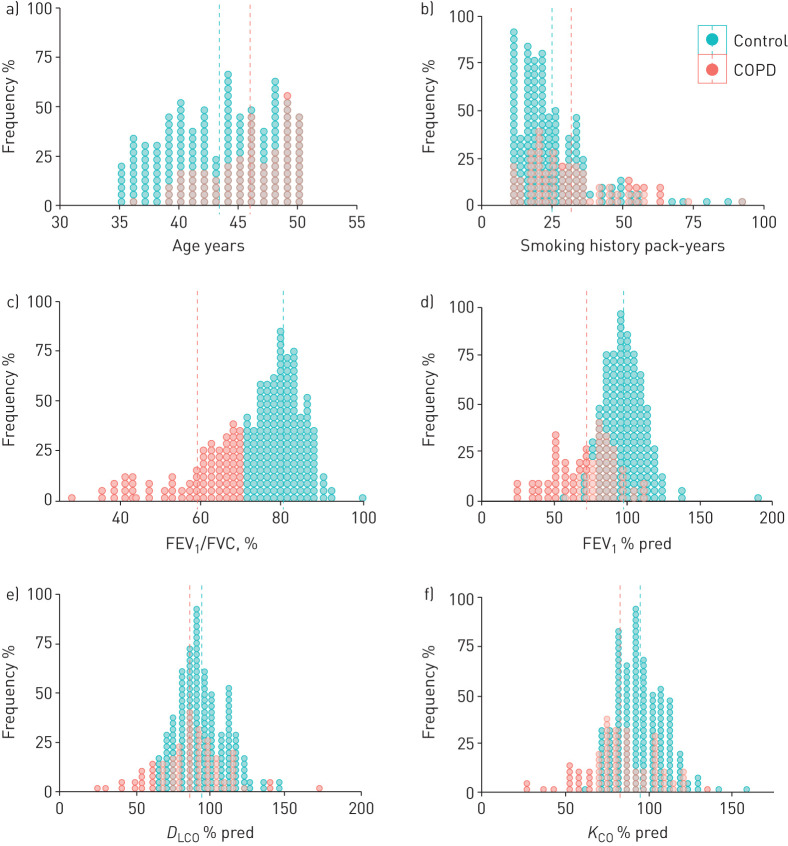
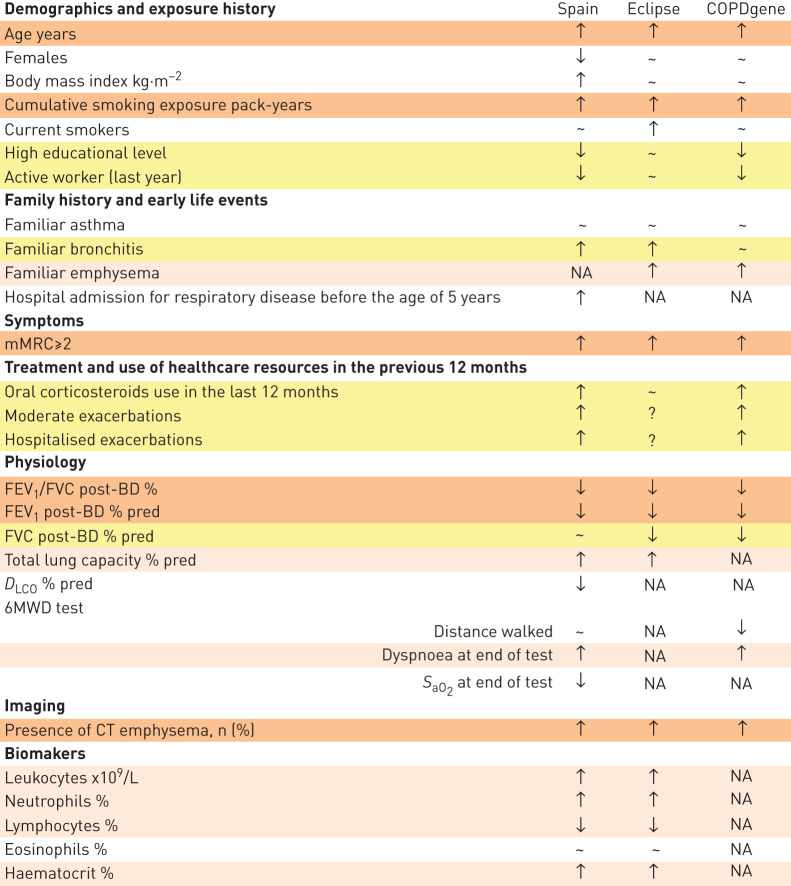
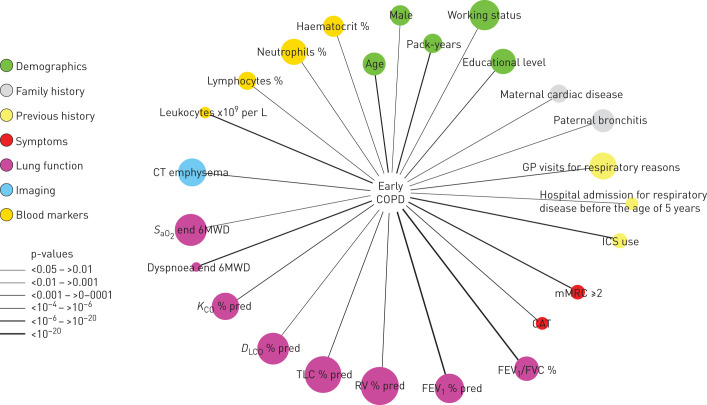
The phenotypic characteristics of chronic obstructive pulmonary disease (COPD) in individuals younger than 50 years of age (early COPD) are not well defined. This prospective, multicentre, case-control study sought to describe these characteristics and compare them with those of smokers (≥10 pack-years) of similar age with normal spirometry (controls). We studied 92 cases (post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <0.7) and 197 controls. Results were contrasted with participants with similar inclusion criteria recruited into the ECLIPSE and COPDGene cohorts. Cases had moderate airflow limitation (FEV1 71.3±20.8%) but were often symptomatic, used healthcare resources frequently, had air trapping (residual volume 150.6±55.5% ref.), had reduced diffusing capacity (84.2±20.7% ref.) and had frequent evidence of computed tomography (CT) emphysema (61%). Of note, less than half of cases (46%) had been previously diagnosed with COPD. Interestingly, they also often reported a family history of respiratory diseases and had been hospitalised because of respiratory problems before the age of 5 years more frequently than controls (12% versus 3%, p=0.009). By and large, these observations were reproduced when available in the ECLIPSE and COPDGene cohorts. These results show that early COPD is associated with substantial health impact and significant structural and functional abnormalities, albeit it is often not diagnosed (hence, treated). The fact that a sizeable proportion of patients with early COPD report a family history of respiratory diseases and/or early-life events (including hospitalisations before the age of 5 years) renders further support to the possibility of early-life origin of COPD.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: B.G. Cosío reports speaker fees from AstraZeneca, grants from Boehringer, grants and speaker fees from Novartis, grants and speaker fees from Chiesi, speaker fees from Rovi, grants from Menarini, and advisory board fees from Esteve, outside the submitted work. Conflict of interest: S. Pascual-Guardia has nothing to disclose. Conflict of interest: A. Borras-Santos has nothing to disclose. Conflict of interest: G. Peces-Barba has nothing to disclose. Conflict of interest: S. Santos reports personal fees from Almirall, Boehringer Ingelheim, AstraZeneca, Gebro Pharma, GlaxoSmithKline, Novartis, Faes, Grifols and Menarini outside the submitted work. Conflict of interest: L. Vigil reports to have received lectures from Boehringer-Ingelheim, GSK, Esteve, Menarini, Novartis, Chiesi and Pfizer. Conflict of interest: J.J. Soler-Cataluña reports personal fees from AstraZeneca, personal fees and non-financial support from Boehringer-Ingelheim, personal fees from Bial, grants and personal fees from GSK, grants, personal fees and non-financial support from Novartis, personal fees from Ferrer, personal fees and non-financial support from Menarini, personal fees from Teva, grants and personal fees from Esteve, outside the submitted work. Conflict of interest: C. Martínez-González reports in the last three years, a grant from Roche Pharma. Conflict of interest: C. Casanova declares in the last three years to have received lectures and/or scientific advice from Laboratorios Bial, Boehringer-Ingelheim, Gebropharma, GSK, Esteve, Menarini, Novartis and Rovi. Conflict of interest: P.J. Marcos reports personal fees from GSK, personal fees from Boehringer Ingelheim, personal fees from Ferrer, personal fees from Menarini and personal fees from Esteve, outside the submitted work. Conflict of interest: C.J. Alvarez has nothing to disclose. Conflict of interest: J.L. López-Campos reports personal fees and non-financial support from AstraZeneca, grants, personal fees and non-financial support from Boehringer Ingelheim, grants, personal fees and non-financial support from Chiesi, personal fees and non-financial support from CSL Behring, grants, personal fees and non-financial support from Esteve, personal fees from Ferrer, grants, personal fees and non-financial support from Gebro Pharma, grants, personal fees and non-financial support from GlaxoSmithKline, grants, personal fees and non-financial support from Grifols, grants, personal fees and non-financial support from Menarini, grants, personal fees and non-financial support from Novartis, grants, personal fees and non-financial support from Rovi, personal fees from Teva, outside the submitted work. Conflict of interest: J. Gea reports grants from Menarini, and advisory board fees from AstraZeneca, GSK and Boehringer Ingelheim, outside the submitted work. Conflict of interest: J. Garcia-Aymerich has nothing to disclose. Conflict of interest: J. Molina reports personal fees from Astra-Zeneca, personal fees from Boehringer-Ingelheim, personal fees from Chiesi, grants and personal fees from GSK, personal fees from Menarini, personal fees from Mundipharma, personal fees from Novartis, personal fees from Pfizer, outside the submitted work. Conflict of interest: M. Román reports personal fees from AstraZeneca, personal fees from Boehringer-Ingelheim, personal fees from Chiesi, grants and personal fees from GSK, personal fees from Menarini, personal fees from Mundipharma, personal fees from Novartis, personal fees from Pfizer, personal fees from Teva, personal fees from Bial, outside the submitted work. Conflict of interest: J. Moises has nothing to disclose. Conflict of interest: V. Szabo has nothing to disclose. Conflict of interest: E.A. Regan has no conflicts. Conflict of interest: R. San José Estépar reports grants from NHLBI, personal fees from Toshiba, personal fees from Boehringer Ingelheim, personal fees from Eolo Medical, personal fees from Leuko Labs, outside the submitted work; and he is also a founder and co-owner of Quantitative Imaging Solutions which is a company that provides image based consulting and develops software to enable data sharing. Conflict of interest: G. Washko reports grants from the NIH; a grant from, and consultancy and advisory board membership for Boehringer Ingelheim; that he is a founder and co-owner of Quantitative Imaging Solutions, which provides image-based consulting and develops software to enable data sharing; consultancy and chairing a DSMB for PulmonX; a grant from BTG Interventional Medicine; a grant from and consultancy for Janssen Pharmaceuticals; and consultancy for GlaxoSmithKline, all outside the submitted work. Dr Washko's spouse works for Biogen, which is focused on developing therapies for fibrotic lung disease. Conflict of interest: A. Agustí reports personal fees from AstraZeneca, grants and personal fees from Menarini, personal fees from Chiesi, grants and personal fees from GSK, personal fees from Nuvaira, outside the submitted work. Conflict of interest: R. Faner reports grants and personal fees from GSK, a speaker fee from Chiesi, and grants from Menarini, outside the submitted work.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources