

Risk of ambulatory colonoscopy in patients with cirrhosis: a propensity-score matched cohort study
- PMID: 33043119
- PMCID: PMC7541192
- DOI: 10.1055/a-1242-9958
Risk of ambulatory colonoscopy in patients with cirrhosis: a propensity-score matched cohort study
Abstract
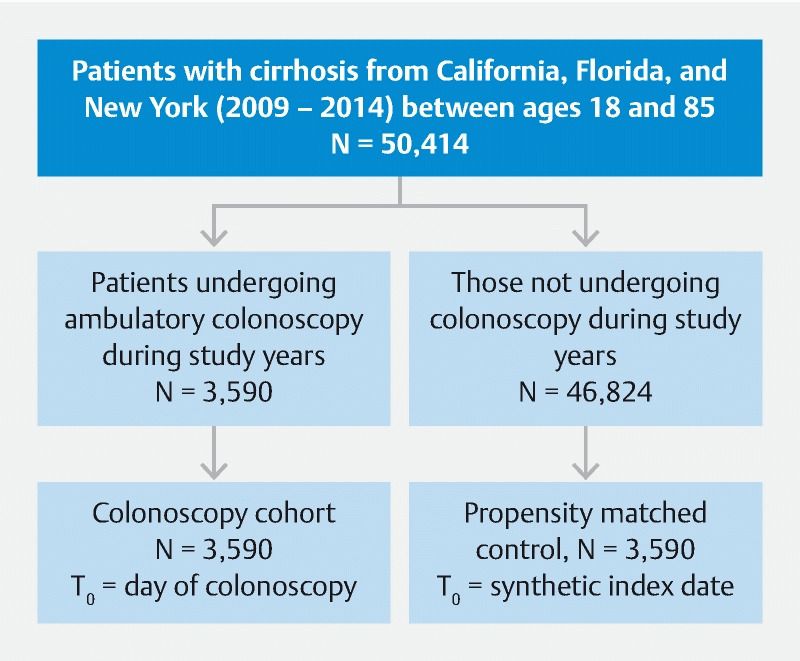
Background and study aims Patients with cirrhosis demonstrate alterations in physiology, hemodynamics, and immunity which may increase procedural risk. There exist sparse data regarding the safety of performing ambulatory colonoscopy in patients with cirrhosis. Patients and methods From a population-based sample of three North American states (California, Florida, and New York), we collected data on 3,590 patients with cirrhosis who underwent ambulatory colonoscopy from 2009 to 2014. We created a control cohort propensity score-matched for cirrhotic severity who did not undergo colonoscopy (N = 3,590) in order to calculate the attributable risk for adverse events. The primary endpoint was the rate of unplanned hospital encounters (UHEs) within 14 days of colonoscopy (or from a synthetic index date for the control cohort). Predictors for UHE were assessed in multivariable regression. Results The attributable risk for any UHE following colonoscopy was 3.1 % (confidence interval [CI] 2.1-4.1 %, P < 0.001). There was increased risk for infection (0.9 %, CI 0.7-1.1 %), spontaneous bacterial peritonitis (0.1 %, CI 0.0-0.3 %), decompensation of ascites (0.3 %, CI 0.2-0.4 %), and cardiovascular event (0.4 %, CI 0.3-0.5 %). There was no increased attributable risk for gastrointestinal bleeding, perforation, or development of the hepatorenal syndrome. The presence of ascites at time of procedure was the only predictor for UHE in the fully-adjusted model (OR 2.6, CI 1.9-3.5, P < 0.001). Conclusions There is a moderate though detectable increase in risk for adverse event following ambulatory colonoscopy in patients with cirrhosis. The presence of ascites in particular portends higher risk. These data may guide clinicians when counseling patients with cirrhosis on the choice of colorectal cancer screening modality.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Unplanned Hospital Encounters After Endoscopic Retrograde Cholangiopancreatography in 3 Large North American States.Gastroenterology. 2019 Jan;156(1):119-129.e3. doi: 10.1053/j.gastro.2018.09.037. Epub 2018 Sep 19. Gastroenterology. 2019. PMID: 30243620 Free PMC article.
-
Low Rates of Gastrointestinal and Non-Gastrointestinal Complications for Screening or Surveillance Colonoscopies in a Population-Based Study.Gastroenterology. 2018 Feb;154(3):540-555.e8. doi: 10.1053/j.gastro.2017.10.006. Epub 2017 Oct 12. Gastroenterology. 2018. PMID: 29031502
-
Early Colonoscopy for Diverticular Bleeding Does Not Reduce Risk of Postdischarge Recurrent Bleeding: A Propensity Score Matching Analysis.Clin Gastroenterol Hepatol. 2019 May;17(6):1105-1111.e1. doi: 10.1016/j.cgh.2018.09.050. Epub 2018 Oct 6. Clin Gastroenterol Hepatol. 2019. PMID: 30296595
-
Proton pump inhibitor use and association with spontaneous bacterial peritonitis in patients with cirrhosis and ascites.Ann Pharmacother. 2012 Oct;46(10):1413-8. doi: 10.1345/aph.1R174. Epub 2012 Oct 2. Ann Pharmacother. 2012. PMID: 23032651 Review.
-
Complications of cirrhosis. II. Renal and circulatory dysfunction. Lights and shadows in an important clinical problem.J Hepatol. 2000;32(1 Suppl):157-70. doi: 10.1016/s0168-8278(00)80423-7. J Hepatol. 2000. PMID: 10728802 Review.
References
-
- Scaglione S, Kliethermes S, Cao G et al.The epidemiology of cirrhosis in the United States: a population-based study. J Clin Gastroenterol. 2015;49:690–696. - PubMed
-
- D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44:217–231. - PubMed
-
- Lieberman D A, Rex D K, Winawer S J et al.Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844–857. - PubMed
-
- Rex D K, Johnson D A, Anderson J C et al.American College of Gastroenterology guidelines for colorectal cancer screening 2009 [corrected] Am J Gastroenterol. 2009;104:739–750. - PubMed
-
- Atassi T, Thuluvath P J. Risk of colorectal adenoma in liver transplant recipients compared to immunocompetent control population undergoing routine screening colonoscopy. J Clin Gastroenterol. 2003;37:72–73. - PubMed
LinkOut - more resources
Full Text Sources