

Machine learning and atherosclerotic cardiovascular disease risk prediction in a multi-ethnic population
- PMID: 33043149
- PMCID: PMC7511400
- DOI: 10.1038/s41746-020-00331-1
Machine learning and atherosclerotic cardiovascular disease risk prediction in a multi-ethnic population
Abstract
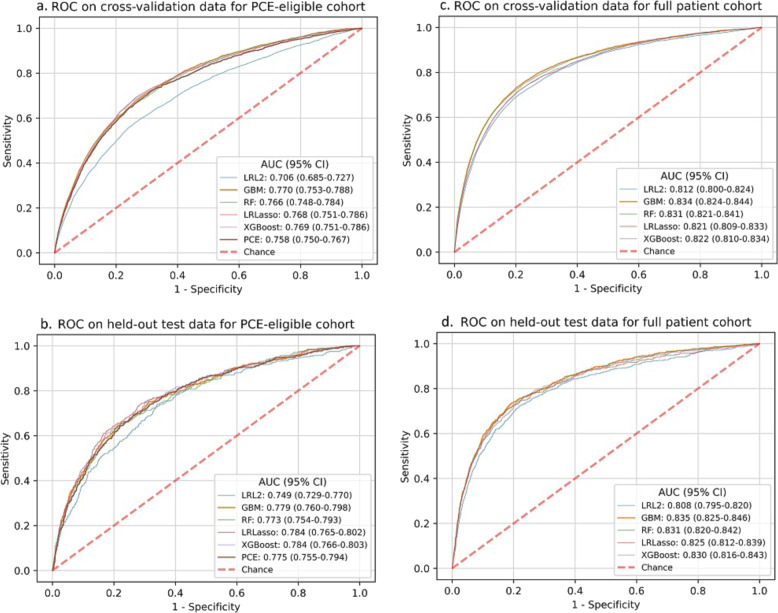
The pooled cohort equations (PCE) predict atherosclerotic cardiovascular disease (ASCVD) risk in patients with characteristics within prespecified ranges and has uncertain performance among Asians or Hispanics. It is unknown if machine learning (ML) models can improve ASCVD risk prediction across broader diverse, real-world populations. We developed ML models for ASCVD risk prediction for multi-ethnic patients using an electronic health record (EHR) database from Northern California. Our cohort included patients aged 18 years or older with no prior CVD and not on statins at baseline (n = 262,923), stratified by PCE-eligible (n = 131,721) or PCE-ineligible patients based on missing or out-of-range variables. We trained ML models [logistic regression with L2 penalty and L1 lasso penalty, random forest, gradient boosting machine (GBM), extreme gradient boosting] and determined 5-year ASCVD risk prediction, including with and without incorporation of additional EHR variables, and in Asian and Hispanic subgroups. A total of 4309 patients had ASCVD events, with 2077 in PCE-ineligible patients. GBM performance in the full cohort, including PCE-ineligible patients (area under receiver-operating characteristic curve (AUC) 0.835, 95% confidence interval (CI): 0.825-0.846), was significantly better than that of the PCE in the PCE-eligible cohort (AUC 0.775, 95% CI: 0.755-0.794). Among patients aged 40-79, GBM performed similarly before (AUC 0.784, 95% CI: 0.759-0.808) and after (AUC 0.790, 95% CI: 0.765-0.814) incorporating additional EHR data. Overall, ML models achieved comparable or improved performance compared to the PCE while allowing risk discrimination in a larger group of patients including PCE-ineligible patients. EHR-trained ML models may help bridge important gaps in ASCVD risk prediction.
Keywords: Cardiovascular diseases; Epidemiology.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures

References
-
- Grundy SM, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019;73:3168–3209. doi: 10.1016/j.jacc.2018.11.002. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
