

Sarilumab use in severe SARS-CoV-2 pneumonia
- PMID: 33043284
- PMCID: PMC7531933
- DOI: 10.1016/j.eclinm.2020.100553
Sarilumab use in severe SARS-CoV-2 pneumonia
Abstract
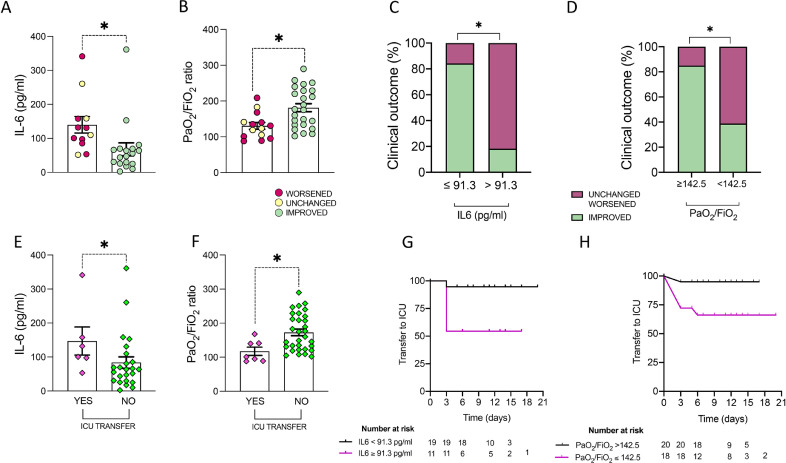
Background: Interleukin-6 signal blockade showed preliminary beneficial effects in treating inflammatory response against SARS-CoV-2 leading to severe respiratory distress. Herein we describe the outcomes of off-label intravenous use of Sarilumab in severe SARS-CoV-2-related pneumonia.
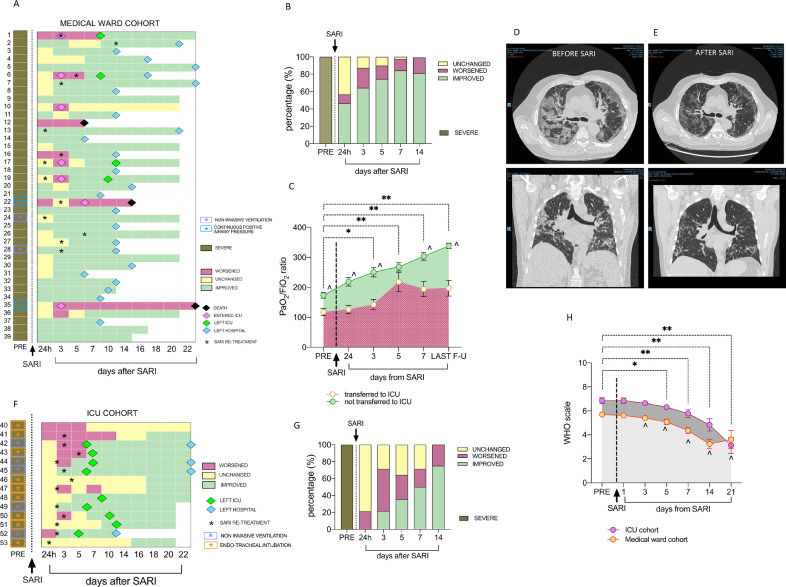
Methods: 53 patients with SARS-CoV-2 severe pneumonia received intravenous Sarilumab; pulmonary function improvement or Intensive Care Unit (ICU) admission rate in medical wards, live discharge rate in ICU treated patients and safety profile were recorded. Sarilumab 400 mg was administered intravenously on day 1, with eventual additional infusion based on clinical judgement, and patients were followed for at least 14 days, unless previously discharged or dead.
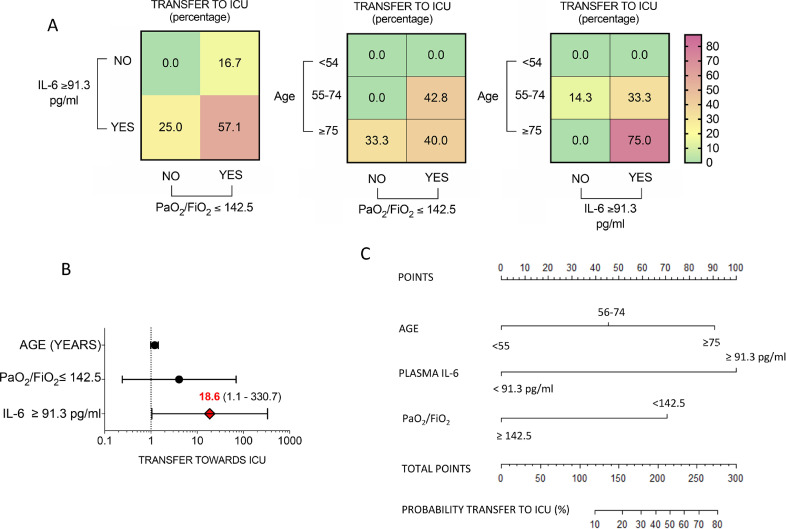
Findings: Of the 53 SARS-CoV-2pos patients receiving Sarilumab, 39(73·6%) were treated in medical wards [66·7% with a single infusion; median PaO2/FiO2:146(IQR:120-212)] while 14(26·4%) in ICU [92·6% with a second infusion; median PaO2/FiO2: 112(IQR:100-141.5)].Within the medical wards, 7(17·9%) required ICU admission, 4 of whom were re-admitted to the ward within 5-8 days. At 19 days median follow-up, 89·7% of medical inpatients significantly improved (46·1% after 24 h, 61·5% after 3 days), 70·6% were discharged from the hospital and 85·7% no longer needed oxygen therapy. Within patients receiving Sarilumab in ICU, 64·2% were discharged from ICU to the ward and 35·8% were still alive at the last follow-up. Overall mortality rate was 5·7%.
Interpretation: IL-6R inhibition appears to be a potential treatment strategy for severe SARS-CoV-2 pneumonia and intravenous Sarilumab seems a promising treatment approach showing, in the short term, an important clinical outcome and good safety.
Keywords: Inflammation; Sarilumab; Severe sars-cov-2 pneumonia.
© 2020 The Authors.
Conflict of interest statement
All authors declare no conflict of interest with the submitted manuscript.
Figures
References
-
- Italian Ministry of Health (www.salute.gov.it)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
