

The utility of high-flow nasal oxygen for severe COVID-19 pneumonia in a resource-constrained setting: A multi-centre prospective observational study
- PMID: 33043285
- PMCID: PMC7536126
- DOI: 10.1016/j.eclinm.2020.100570
The utility of high-flow nasal oxygen for severe COVID-19 pneumonia in a resource-constrained setting: A multi-centre prospective observational study
Abstract
Background: The utility of heated and humidified high-flow nasal oxygen (HFNO) for severe COVID-19-related hypoxaemic respiratory failure (HRF), particularly in settings with limited access to intensive care unit (ICU) resources, remains unclear, and predictors of outcome have been poorly studied.
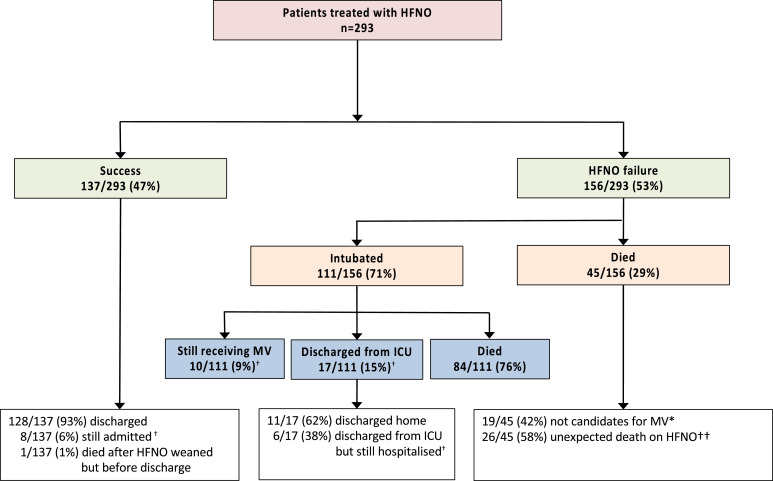
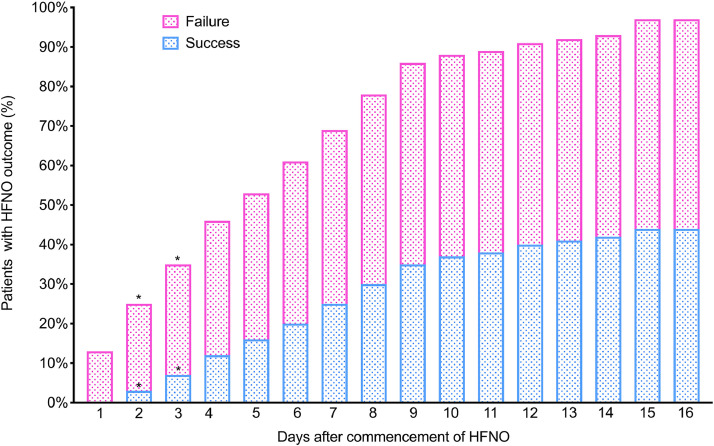
Methods: We included consecutive patients with COVID-19-related HRF treated with HFNO at two tertiary hospitals in Cape Town, South Africa. The primary outcome was the proportion of patients who were successfully weaned from HFNO, whilst failure comprised intubation or death on HFNO.
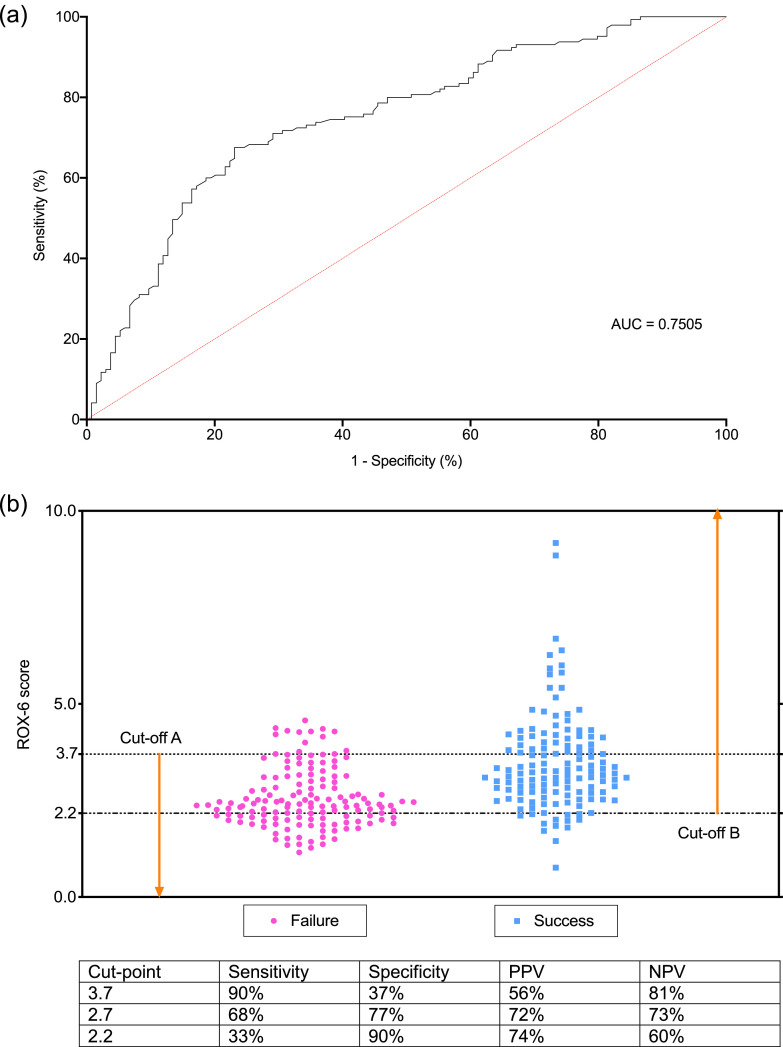
Findings: The median (IQR) arterial oxygen partial pressure to fraction inspired oxygen ratio (PaO2/FiO2) was 68 (54-92) in 293 enroled patients. Of these, 137/293 (47%) of patients [PaO2/FiO2 76 (63-93)] were successfully weaned from HFNO. The median duration of HFNO was 6 (3-9) in those successfully treated versus 2 (1-5) days in those who failed (p<0.001). A higher ratio of oxygen saturation/FiO2 to respiratory rate within 6 h (ROX-6 score) after HFNO commencement was associated with HFNO success (ROX-6; AHR 0.43, 0.31-0.60), as was use of steroids (AHR 0.35, 95%CI 0.19-0.64). A ROX-6 score of ≥3.7 was 80% predictive of successful weaning whilst ROX-6 ≤ 2.2 was 74% predictive of failure. In total, 139 patents (52%) survived to hospital discharge, whilst mortality amongst HFNO failures with outcomes was 129/140 (92%).
Interpretation: In a resource-constrained setting, HFNO for severe COVID-19 HRF is feasible and more almost half of those who receive it can be successfully weaned without the need for mechanical ventilation.
Keywords: COVID-19; High flow nasal oxygen; Pneumonia; Ventilation.
© 2020 The Author(s).
Conflict of interest statement
BA has received speakers fees from Novartis, and CK has served on an advisory board from AstraZeneca, both outside the submitted work.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
