

Application of percutaneous transluminal sharp recanalization in transjugular intrahepatic portosystemic shunt for patients with chronic portal vein occlusion
- PMID: 33044172
- PMCID: PMC7963390
- DOI: 10.5152/dir.2020.20461
Application of percutaneous transluminal sharp recanalization in transjugular intrahepatic portosystemic shunt for patients with chronic portal vein occlusion
Abstract
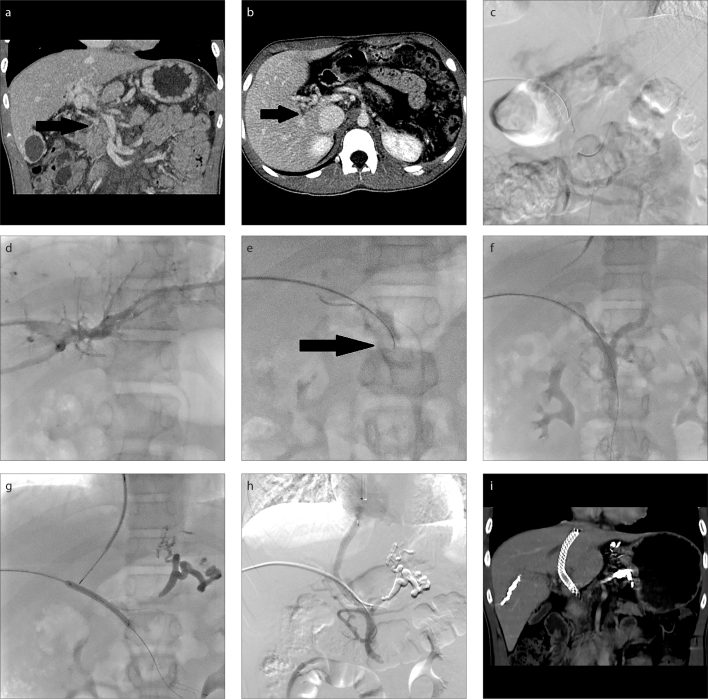
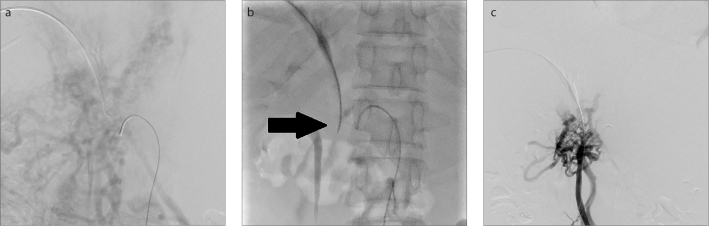
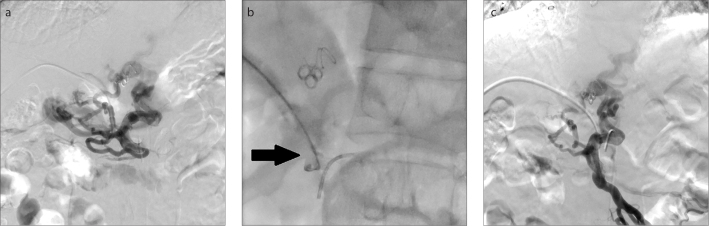
Purpose: We aimed to evaluate the feasibility and safety of a modified technique for portal vein recanalization, percutaneous transluminal sharp recanalization (PTSR), when performing transjugular intrahepatic portosystemic shunt (TIPS) for the treatment of chronic portal vein occlusion (CPVO) and portal hypertension.
Methods: Nine consecutive patients with CPVO and portal hypertension had undergone TIPS and PTSR procedure after failing in conventional percutaneous catheterization from March 2017 to July 2019. Technical success rates, effectiveness, and complications were evaluated. Follow-up of patients' clinical outcomes and shunt patency were performed periodically. Primary and secondary shunt patency were analyzed by Kaplan-Meier method.
Results: The occluded portal veins were successfully recanalized after failing in conventional percutaneous catheterization, and TIPS procedures were completed in all 9 patients. Two patients suffered from procedure-related complications. A portosystemic pressure gradient <12 mmHg, or a percent reduction of 25% to 50% of baseline, was achieved in all 9 patients after TIPS. During the median follow-up period of 28 months (range, 9-36 months), 1 patient experienced recurrent ascites and the other 8 patients remained asymptomatic. The cumulative rates of primary and secondary shunt patency were 66.67% and 100%, respectively, at 2 years.
Conclusion: As a supplementary method, PTSR is a feasible and safe method for portal vein recanalization when performing TIPS for patients with CPVO and portal hypertension.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
