

Multicenter analysis of sputum microbiota in tuberculosis patients
- PMID: 33044973
- PMCID: PMC7549818
- DOI: 10.1371/journal.pone.0240250
Multicenter analysis of sputum microbiota in tuberculosis patients
Abstract
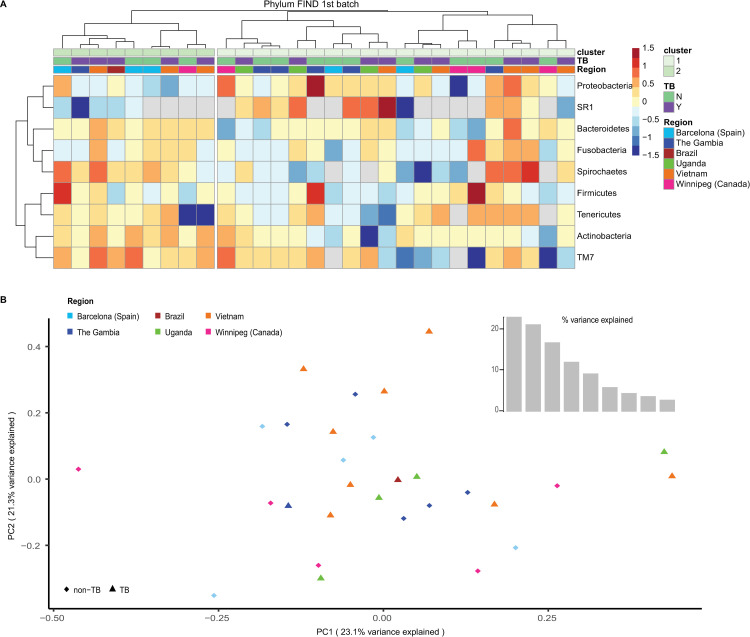
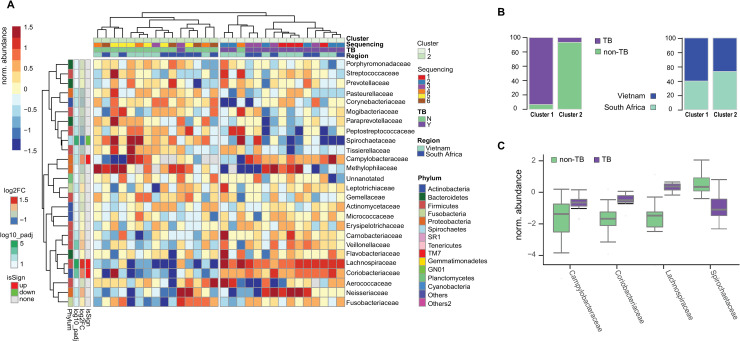
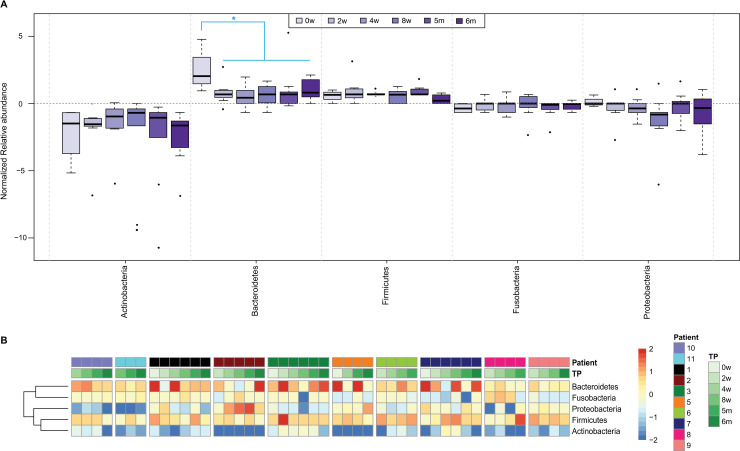
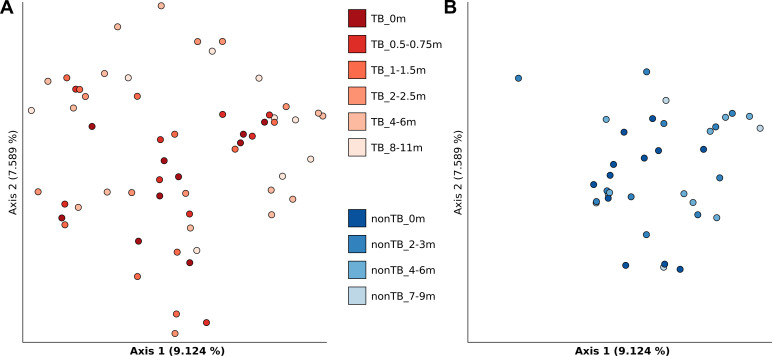
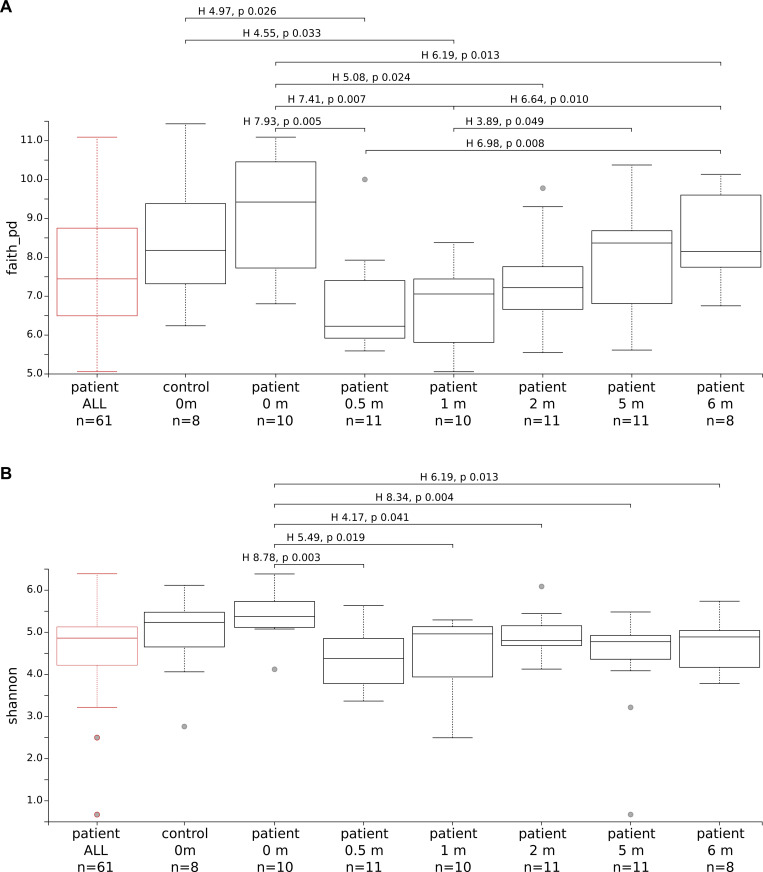
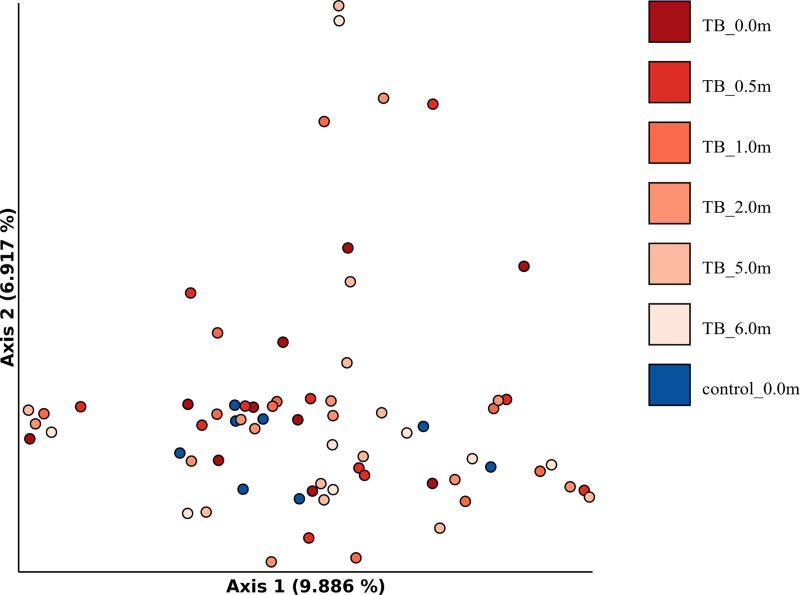
The impact of tuberculosis and of anti-tuberculosis therapy on composition and modification of human lung microbiota has been the object of several investigations. However, no clear outcome has been presented so far and the relationship between M. tuberculosis pulmonary infection and the resident lung microbiota remains vague. In this work we describe the results obtained from a multicenter study of the microbiota of sputum samples from patients with tuberculosis or unrelated lung diseases and healthy donors recruited in Switzerland, Italy and Bangladesh, with the ultimate goal of discovering a microbiota-based biomarker associated with tuberculosis. Bacterial 16S rDNA amplification, high-throughput sequencing and extensive bioinformatic analyses revealed patient-specific flora and high variability in taxon abundance. No common signature could be identified among the individuals enrolled except for minor differences which were not consistent among the different geographical settings. Moreover, anti-tuberculosis therapy did not cause any important variation in microbiota diversity, thus precluding its exploitation as a biomarker for the follow up of tuberculosis patients undergoing treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Global Tuberculosis Report 2019. 2019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
