

Polypharmacy in Older Adults Hospitalized for Heart Failure
- PMID: 33045844
- PMCID: PMC8819498
- DOI: 10.1161/CIRCHEARTFAILURE.120.006977
Polypharmacy in Older Adults Hospitalized for Heart Failure
Abstract
Background: Despite potential harm that can result from polypharmacy, real-world data on polypharmacy in the setting of heart failure (HF) are limited. We sought to address this knowledge gap by studying older adults hospitalized for HF derived from the REGARDS study (Reasons for Geographic and Racial Differences in Stroke).
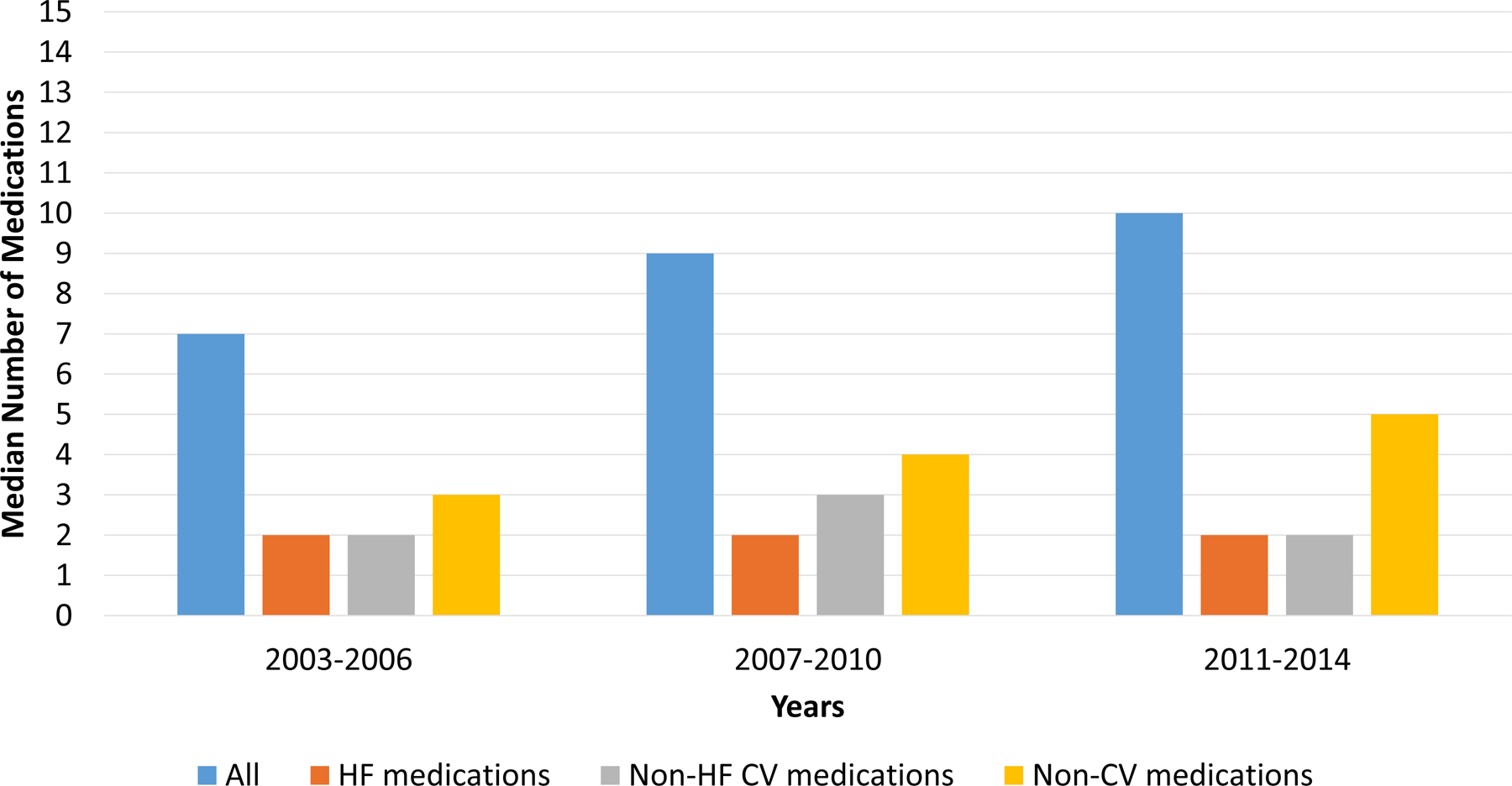
Methods: We examined 558 older adults aged ≥65 years with adjudicated HF hospitalizations from 380 hospitals across the United States. We collected and examined data from the REGARDS baseline assessment, medical charts from HF-adjudicated hospitalizations, the American Hospital Association annual survey database, and Medicare's Hospital Compare website. We counted the number of medications taken at hospital admission and discharge; and classified each medication as HF-related, non-HF cardiovascular-related, or noncardiovascular-related.
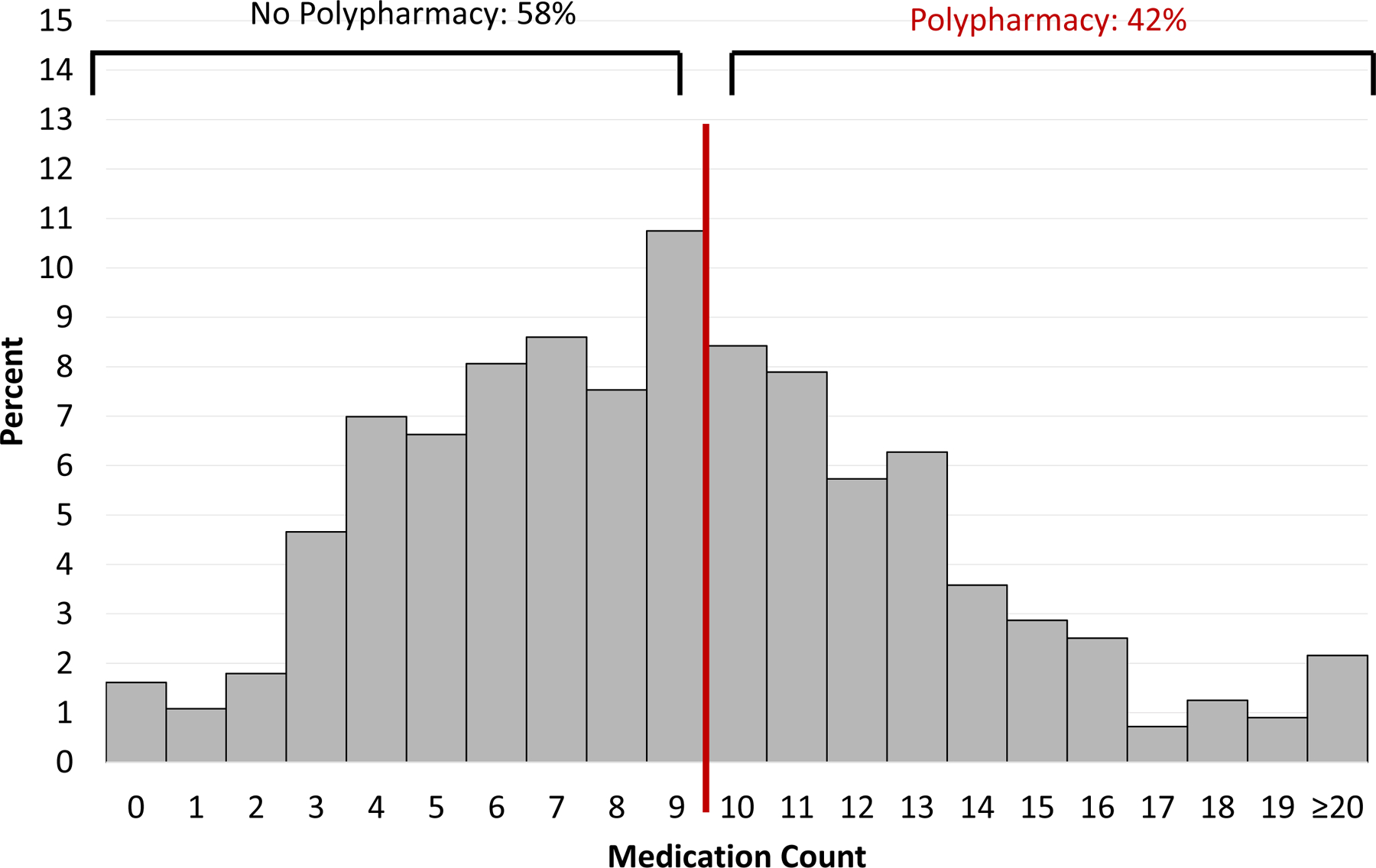
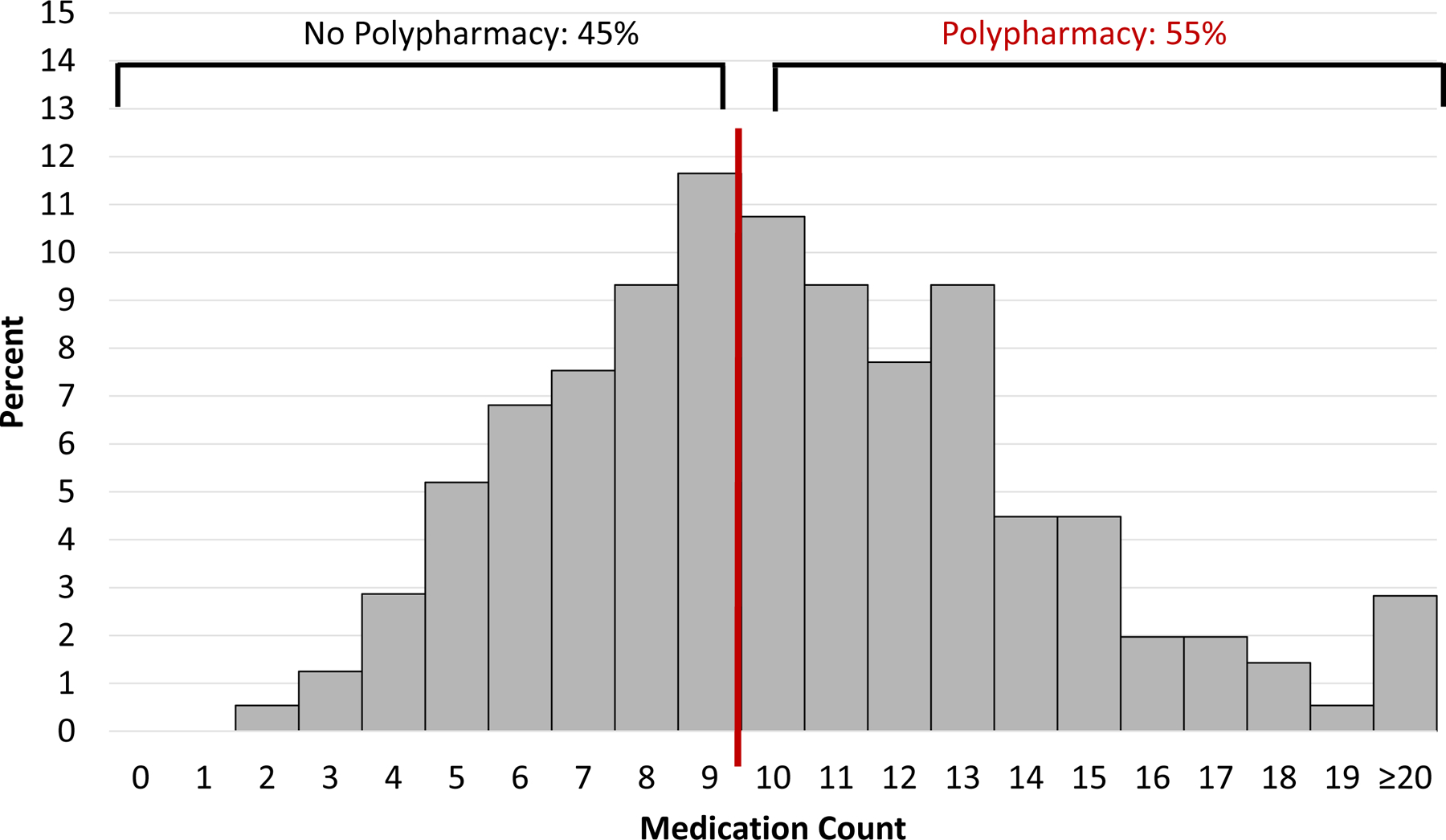
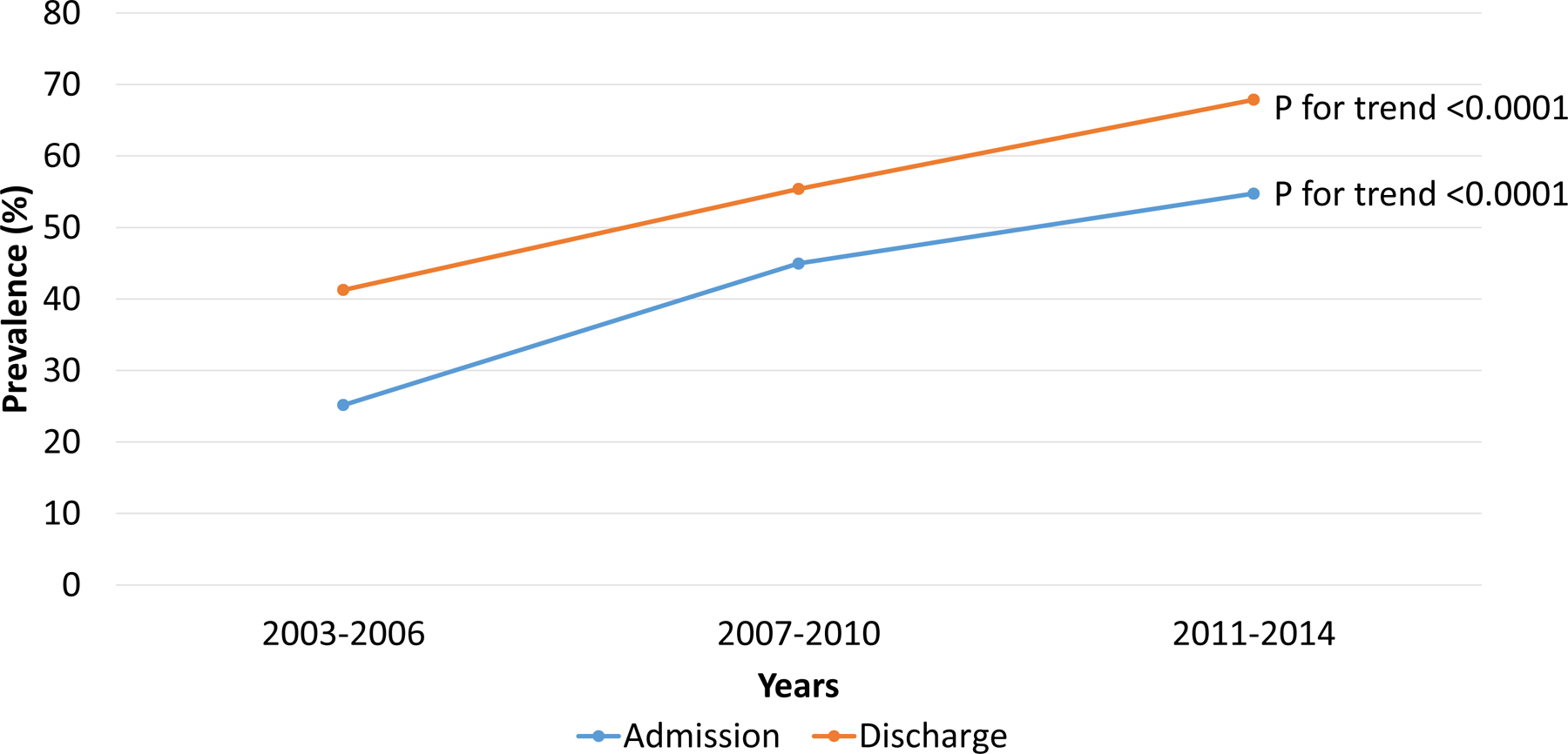
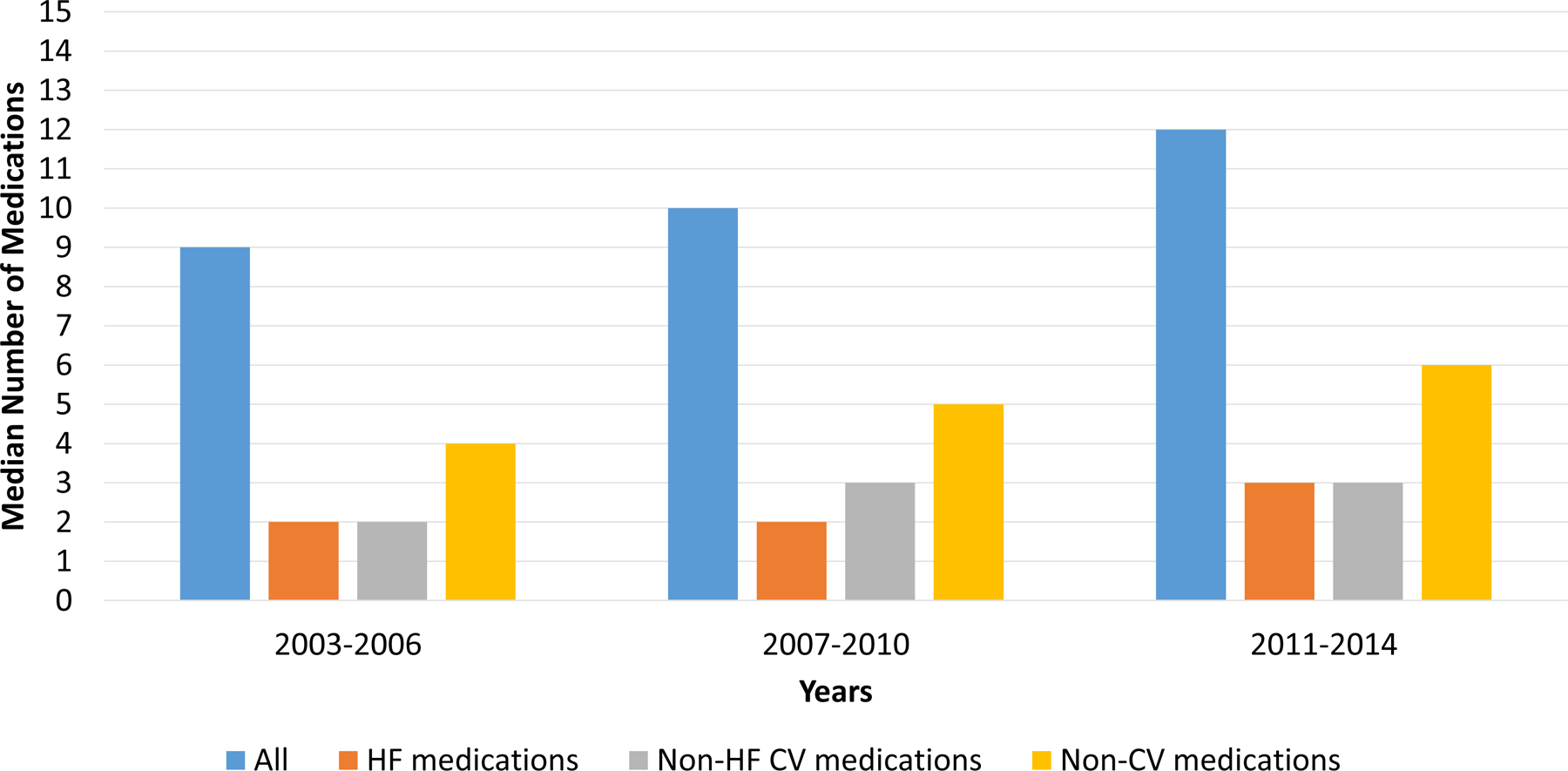
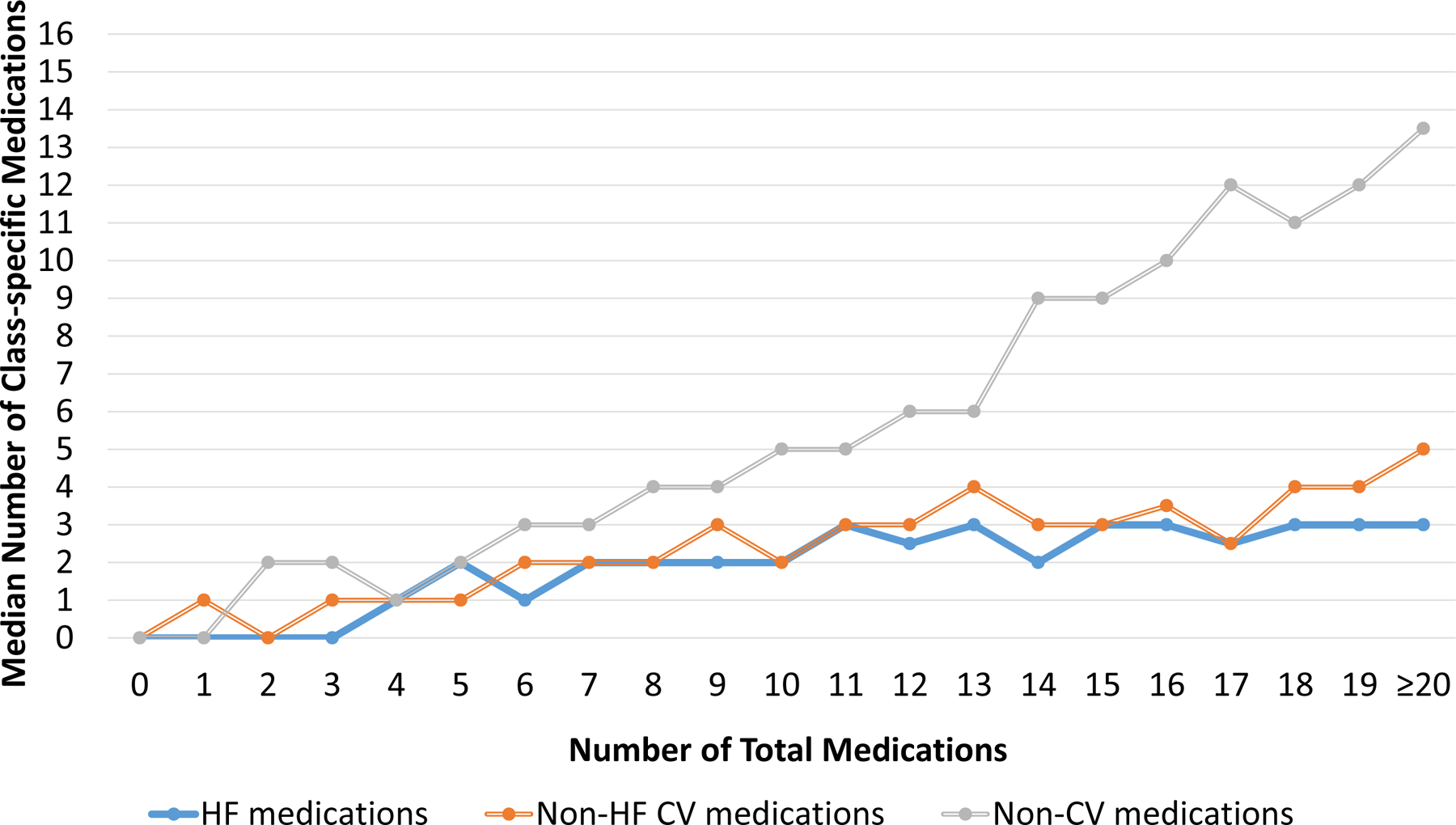
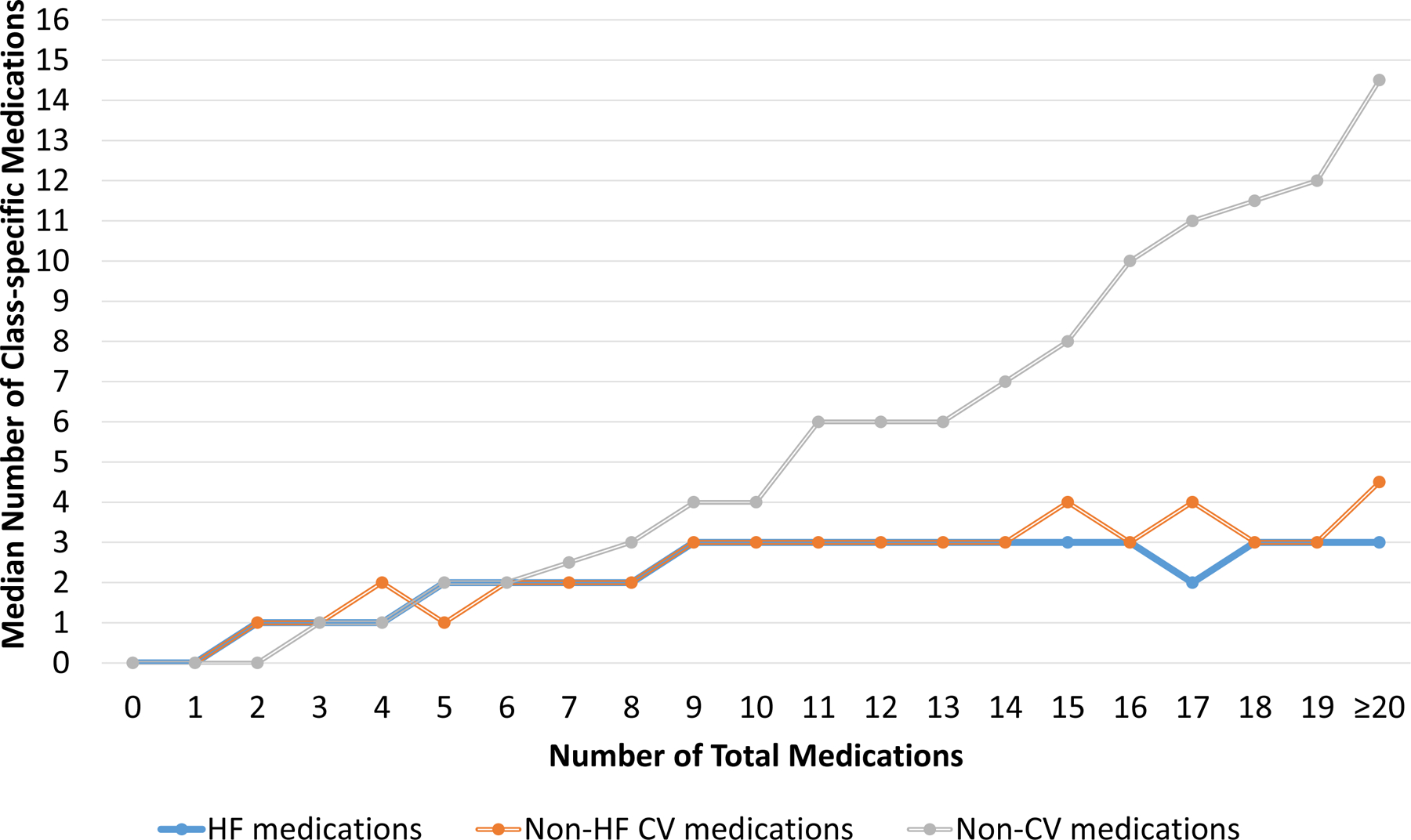
Results: The vast majority of participants (84% at admission and 95% at discharge) took ≥5 medications; and 42% at admission and 55% at discharge took ≥10 medications. The prevalence of taking ≥10 medications (polypharmacy) increased over the study period. As the number of total medications increased, the number of noncardiovascular medications increased more rapidly than the number of HF-related or non-HF cardiovascular medications.
Conclusions: Defining polypharmacy as taking ≥10 medications might be more ideal in the HF population as most patients already take ≥5 medications. Polypharmacy is common both at admission and hospital discharge, and its prevalence is rising over time. The majority of medications taken by older adults with HF are noncardiovascular medications. There is a need to develop strategies that can mitigate the negative effects of polypharmacy among older adults with HF.
Keywords: heart failure; hospitalization; polypharmacy; prevalence.
Figures
Comment in
-
Heart Failure Medical Management in 2020: Searching for the Right Polypharmacy.Circ Heart Fail. 2020 Nov;13(11):e007779. doi: 10.1161/CIRCHEARTFAILURE.120.007779. Epub 2020 Oct 13. Circ Heart Fail. 2020. PMID: 33045846 No abstract available.
-
Response by Unlu et al to Letter Regarding Article, "Polypharmacy in Older Adults Hospitalized for Heart Failure".Circ Heart Fail. 2021 Mar;14(3):e008305. doi: 10.1161/CIRCHEARTFAILURE.121.008305. Epub 2021 Mar 12. Circ Heart Fail. 2021. PMID: 33706544 Free PMC article. No abstract available.
-
Letter by Cogswell et al Regarding Article, "Polypharmacy in Older Adults Hospitalized for Heart Failure".Circ Heart Fail. 2021 Mar;14(3):e008160. doi: 10.1161/CIRCHEARTFAILURE.120.008160. Epub 2021 Mar 12. Circ Heart Fail. 2021. PMID: 33706550 No abstract available.
References
-
- McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Belohlavek J, Bohm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukat A, Ge J, Howlett JG, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Petrie MC, Vinh PN, Schou M, Tereshchenko S, Verma S, Held C, DeMets DL, Docherty KF, Jhund PS, Bengtsson O, Sjostrand M, Langkilde AM, Committees D-HT and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019;381:1995–2008. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ and Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128:1810–52. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW and Westlake C. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017. - PubMed
-
- Centers for Medicare & Medicaid Services. Chronic Conditions among Medicare Beneficiaries. Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Tren... Accessed February 18, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
