

Relationship between the bony correction angle and mechanical axis change and their differences between closed and open wedge high tibial osteotomy
- PMID: 33046054
- PMCID: PMC7549202
- DOI: 10.1186/s12891-020-03703-6
Relationship between the bony correction angle and mechanical axis change and their differences between closed and open wedge high tibial osteotomy
Abstract
Background: The purpose of this study was to investigate the relationship between the bony correction angle and mechanical axis change and their differences between closed wedge high tibial osteotomy (CWHTO) and open wedge high tibial osteotomy (OWHTO).
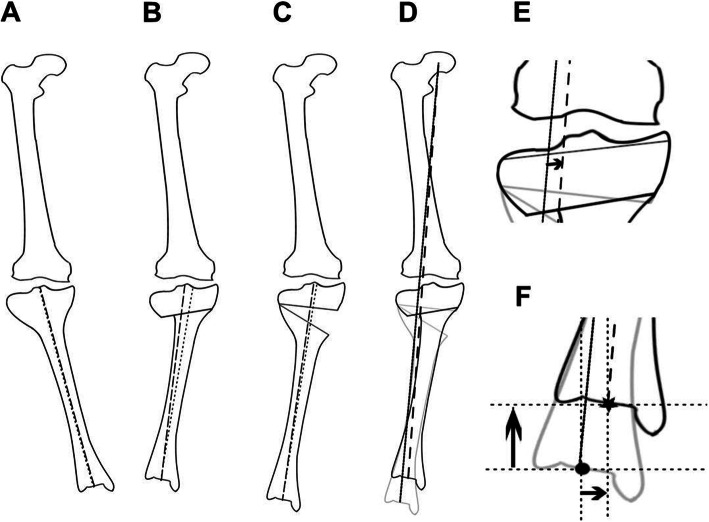
Methods: A total of 100 knees of 89 patients who underwent OWHTO (50 knees) or CWHTO (50 knees) between 2011 and 2015 with a clinical follow-up for 1 year and a radiological follow-up for 1 month were investigated in a case control study. Anteroposterior radiographs of the knee and full-length leg were taken in the standing position using digital acquisition. The femorotibial angle (FTA), % mechanical axis deviation (MAD), % anatomical tibial axis deviation (ATAD), % mechanical tibial axis deviation (MTAD), mechanical medial proximal tibial angle (mMPTA), and joint line convergence angle (JLCA) were measured on preoperative and postoperative radiographs using a dedicated software.
Results: CWHTO resulted in a greater variation between the tibial anatomical and mechanical axes than OWHTO (P < 0.05), and a greater soft tissue correction than OWHTO (P < 0.05). However, no significant difference was found between CWHTO and OWHTO in the ratio of MAD change to the correction angle. When the osteotomy was planned with the same bony correction angle, %MAD passed more laterally in OWHTO than in CWHTO (P < 0.05). These results suggested a lesser valgus bony correction ratio due to greater medial shift of the tibial axis and greater valgus compensation of the soft tissue in CWHTO compared to OWHTO.
Conclusions: The ratio of mechanical axis shift to the correction angle differed in preoperative planning, but postoperative alignment was comparable between opening wedge and closed wedge high tibial osteotomy.
Keywords: Closed wedge; Correction angle; High tibial osteotomy; Mechanical axis shift; Opening wedge.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Difference in the early postoperative change of the joint line convergence angle between opening wedge and closed wedge high tibial osteotomies.J Orthop Surg Res. 2021 Jan 19;16(1):66. doi: 10.1186/s13018-021-02214-x. J Orthop Surg Res. 2021. PMID: 33468195 Free PMC article.
-
Patellofemoral Cartilage Degeneration After Closed- and Open-Wedge High Tibial Osteotomy With Large Alignment Correction.Am J Sports Med. 2020 Sep;48(11):2718-2725. doi: 10.1177/0363546520943872. Epub 2020 Aug 7. Am J Sports Med. 2020. PMID: 32762564
-
Lower Limb Length Discrepancy After High Tibial Osteotomy: Prospective Randomized Controlled Trial of Lateral Closing Versus Medial Opening Wedge Osteotomy.Am J Sports Med. 2016 Dec;44(12):3095-3102. doi: 10.1177/0363546516659284. Epub 2016 Aug 8. Am J Sports Med. 2016. PMID: 27501836 Clinical Trial.
-
Radiographic changes and clinical outcomes after open and closed wedge high tibial osteotomy: a systematic review and meta-analysis.J Orthop Surg Res. 2019 Jun 14;14(1):179. doi: 10.1186/s13018-019-1222-x. J Orthop Surg Res. 2019. PMID: 31200743 Free PMC article.
-
Is opening-wedge high tibial osteotomy superior to closing-wedge high tibial osteotomy in treatment of unicompartmental osteoarthritis? A meta-analysis of randomized controlled trials.Int J Surg. 2018 Dec;60:153-163. doi: 10.1016/j.ijsu.2018.10.045. Epub 2018 Nov 13. Int J Surg. 2018. PMID: 30445197 Review.
Cited by
-
High tibial osteotomy improves balance control in patients with knee osteoarthritis and a varus deformity.J Orthop Surg Res. 2023 Jul 28;18(1):538. doi: 10.1186/s13018-023-04041-8. J Orthop Surg Res. 2023. PMID: 37507811 Free PMC article.
-
Osteotomies and Total Knee Arthroplasty: Systematic Review and Meta-Analysis.Life (Basel). 2022 Jul 26;12(8):1120. doi: 10.3390/life12081120. Life (Basel). 2022. PMID: 35892922 Free PMC article. Review.
-
Lateral closing wedge high tibial osteotomy procedure for the treatment of medial knee osteoarthritis: eleven years mean follow up analysis.Int Orthop. 2025 Jul;49(7):1655-1666. doi: 10.1007/s00264-025-06525-0. Epub 2025 Apr 23. Int Orthop. 2025. PMID: 40266312 Free PMC article.
-
Potential anatomic risk factors resulting oversized postoperative medial proximal tibial angle after double level osteotomy.BMC Musculoskelet Disord. 2022 Dec 23;23(1):1121. doi: 10.1186/s12891-022-06101-2. BMC Musculoskelet Disord. 2022. PMID: 36550449 Free PMC article.
-
Difference in Correction Power between Hybrid Lateral Closed-Wedge High Tibial Osteotomy and Medial Open-Wedge High Tibial Osteotomy was Associated with Severity of Varus Deformity and Different Hinge Distance from Center of Deformity.Diagnostics (Basel). 2024 May 29;14(11):1137. doi: 10.3390/diagnostics14111137. Diagnostics (Basel). 2024. PMID: 38893663 Free PMC article.
References
-
- Duivenvoorden T, Brouwer RW, Baan A, Bos PK, Reijman M, Bierma-Zeinstra SM, et al. Comparison of closing-wedge and opening-wedge high tibial osteotomy for medial compartment osteoarthritis of the knee: a randomized controlled trial with a six-year follow-up. J Bone Joint Surg Am. 2014;96:1425–1432. doi: 10.2106/JBJS.M.00786. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
