

Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis
- PMID: 33047295
- PMCID: PMC7549421
- DOI: 10.1007/s11547-020-01293-w
Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis
Erratum in
-
Correction to: Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis.Radiol Med. 2021 Apr;126(4):643. doi: 10.1007/s11547-020-01322-8. Radiol Med. 2021. PMID: 33387298 Free PMC article. No abstract available.
Abstract
Objective: To evaluate by means of regression models the relationships between baseline clinical and laboratory data and lung involvement on baseline chest CT and to quantify the thoracic disease using an artificial intelligence tool and a visual scoring system to predict prognosis in patients with COVID-19 pneumonia.
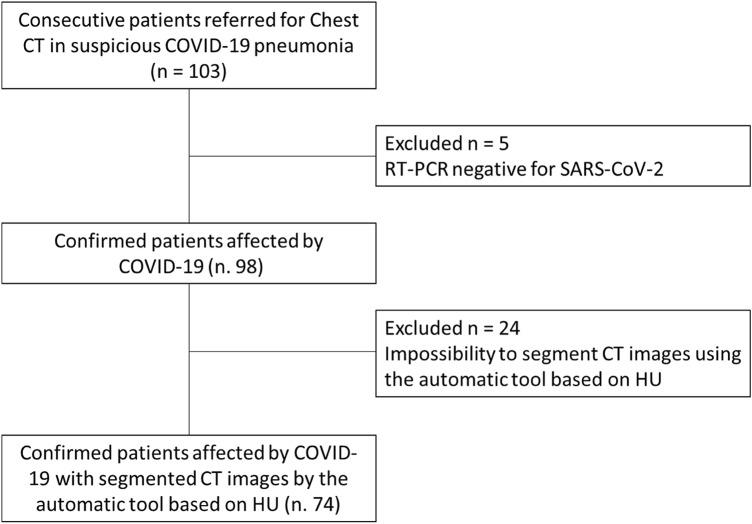
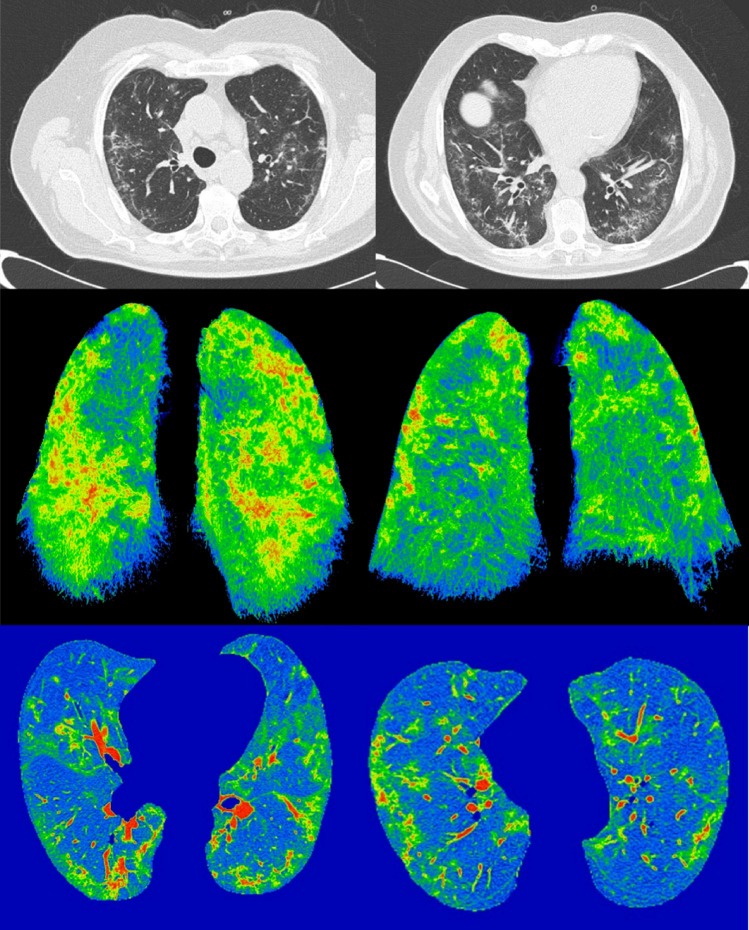
Materials and methods: This study included 103 (41 women and 62 men; 68.8 years of mean age-range, 29-93 years) with suspicious COVID-19 viral infection evaluated by reverse transcription real-time fluorescence polymerase chain reaction (RT-PCR) test. All patients underwent CT examinations at the time of admission in addition to clinical and laboratory findings recording. All chest CT examinations were reviewed using a structured report. Moreover, using an artificial intelligence tool we performed an automatic segmentation on CT images based on Hounsfield unit to calculate residual healthy lung parenchyma, ground-glass opacities (GGO), consolidations and emphysema volumes for both right and left lungs. Two expert radiologists, in consensus, attributed at the CT pulmonary disease involvement a severity score using a scale of 5 levels; the score was attributed for GGO and consolidation for each lung, and then, an overall radiological severity visual score was obtained summing the single score. Univariate and multivariate regression analysis was performed.
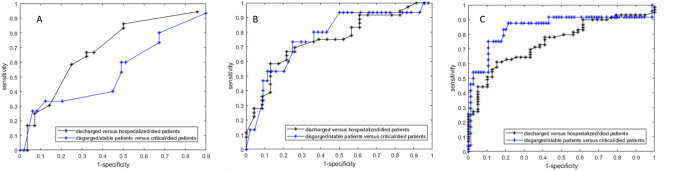
Results: Symptoms and comorbidities did not show differences statistically significant in terms of patient outcome. Instead, SpO2 was significantly lower in patients hospitalized in critical conditions or died while age, HS CRP, leukocyte count, neutrophils, LDH, d-dimer, troponin, creatinine and azotemia, ALT, AST and bilirubin values were significantly higher. GGO and consolidations were the main CT patterns (a variable combination of GGO and consolidations was found in 87.8% of patients). CT COVID-19 disease was prevalently bilateral (77.6%) with peripheral distribution (74.5%) and multiple lobes localizations (52.0%). Consolidation, emphysema and residual healthy lung parenchyma volumes showed statistically significant differences in the three groups of patients based on outcome (patients discharged at home, patients hospitalized in stable conditions and patient hospitalized in critical conditions or died) while GGO volume did not affect the patient's outcome. Moreover, the overall radiological severity visual score (cutoff ≥ 8) was a predictor of patient outcome. The highest value of R-squared (R2 = 0.93) was obtained by the model that combines clinical/laboratory findings at CT volumes. The highest accuracy was obtained by clinical/laboratory and CT findings model with a sensitivity, specificity and accuracy, respectively, of 88%, 78% and 81% to predict discharged/stable patients versus critical/died patients.
Conclusion: In conclusion, both CT visual score and computerized software-based quantification of the consolidation, emphysema and residual healthy lung parenchyma on chest CT images were independent predictors of outcome in patients with COVID-19 pneumonia.
Keywords: COVID-19; Chest CT; Outcome; Regression model.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization website. Middle East respiratory syndrome coronavirus (MERS-CoV). www.who.int/emergencies/mers-cov/en/. Accessed 21 March 2020
-
- World Health Organization website. Naming the coronavirus disease (COVID-2019) and the virus that causes it. www.who.int/emergencies/diseases/. Accessed 21 March 2020
-
- Wuhan Coronavirus (2019-nCoV) Global Cases (by Johns Hopkins CSSE). Case Dashboard. https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594.... Accessed 21 March 2020
-
- American College of Radiology (ACR). ACR Recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 Infection.https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom.... Published March 11, 2020. Accessed 4 April 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
