

T cell and antibody responses to SARS-CoV-2: Experience from a French transplantation and hemodialysis center during the COVID-19 pandemic
- PMID: 33047493
- PMCID: PMC7675512
- DOI: 10.1111/ajt.16348
T cell and antibody responses to SARS-CoV-2: Experience from a French transplantation and hemodialysis center during the COVID-19 pandemic
Abstract
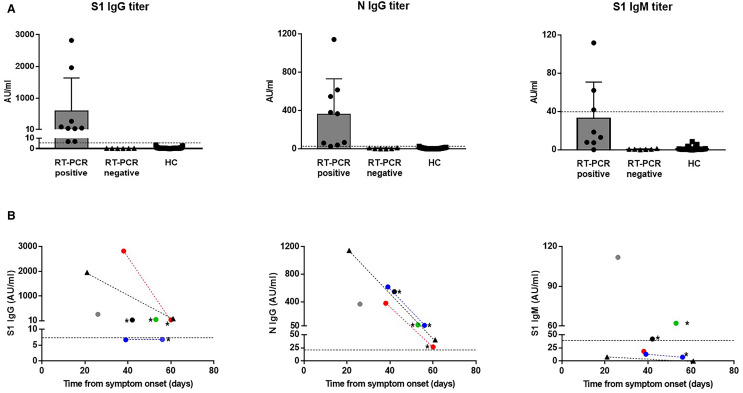
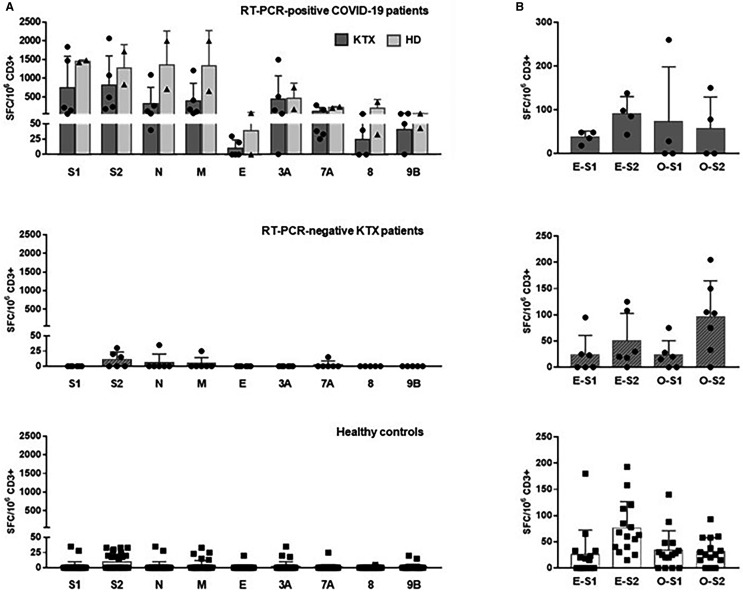
Immunosuppressed organ-transplanted patients are considered at risk for severe forms of COVID-19. Moreover, exaggerated innate and adaptive immune responses might be involved in severe progression of the disease. However, no data on the immune response to SARS-CoV-2 in transplanted patients are currently available. Here, we report the first assessment of antibody and T cell responses to SARS-CoV-2 in 11 kidney-transplanted patients recovered from RT-PCR-confirmed (n = 5) or initially suspected (n = 6) COVID-19. After reduction of immunosuppressive therapy, RT-PCR-confirmed COVID-19 transplant patients were able to mount vigorous antiviral T cell and antibody responses, as efficiently as two nontherapeutically immunosuppressed COVID-19 patients on hemodialysis. By contrast, six RT-PCR-negative patients displayed no antibody response. Among them, three showed very low numbers of SARS-CoV-2-reactive T cells, whereas no T cell response was detected in the other three, potentially ruling out COVID-19 diagnosis. Low levels of T cell reactivity to SARS-CoV-2 were also detected in seronegative healthy controls without known exposure to the virus. These results suggest that during COVID-19, monitoring both T cell and serological immunity might be helpful for the differential diagnosis of COVID-19 but are also needed to evaluate a potential role of antiviral T cells in the development of severe forms of the disease.
Keywords: immunobiology; infection and infectious agents - viral; kidney transplantation / nephrology; monitoring: immune; translational research / science.
© 2020 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
