

Association of Receipt of Palliative Care Interventions With Health Care Use, Quality of Life, and Symptom Burden Among Adults With Chronic Noncancer Illness: A Systematic Review and Meta-analysis
- PMID: 33048152
- PMCID: PMC8094426
- DOI: 10.1001/jama.2020.14205
Association of Receipt of Palliative Care Interventions With Health Care Use, Quality of Life, and Symptom Burden Among Adults With Chronic Noncancer Illness: A Systematic Review and Meta-analysis
Abstract
Importance: The evidence for palliative care exists predominantly for patients with cancer. The effect of palliative care on important end-of-life outcomes in patients with noncancer illness is unclear.
Objective: To measure the association between palliative care and acute health care use, quality of life (QOL), and symptom burden in adults with chronic noncancer illnesses.
Data sources: MEDLINE, Embase, CINAHL, PsycINFO, and PubMed from inception to April 18, 2020.
Study selection: Randomized clinical trials of palliative care interventions in adults with chronic noncancer illness. Studies involving at least 50% of patients with cancer were excluded.
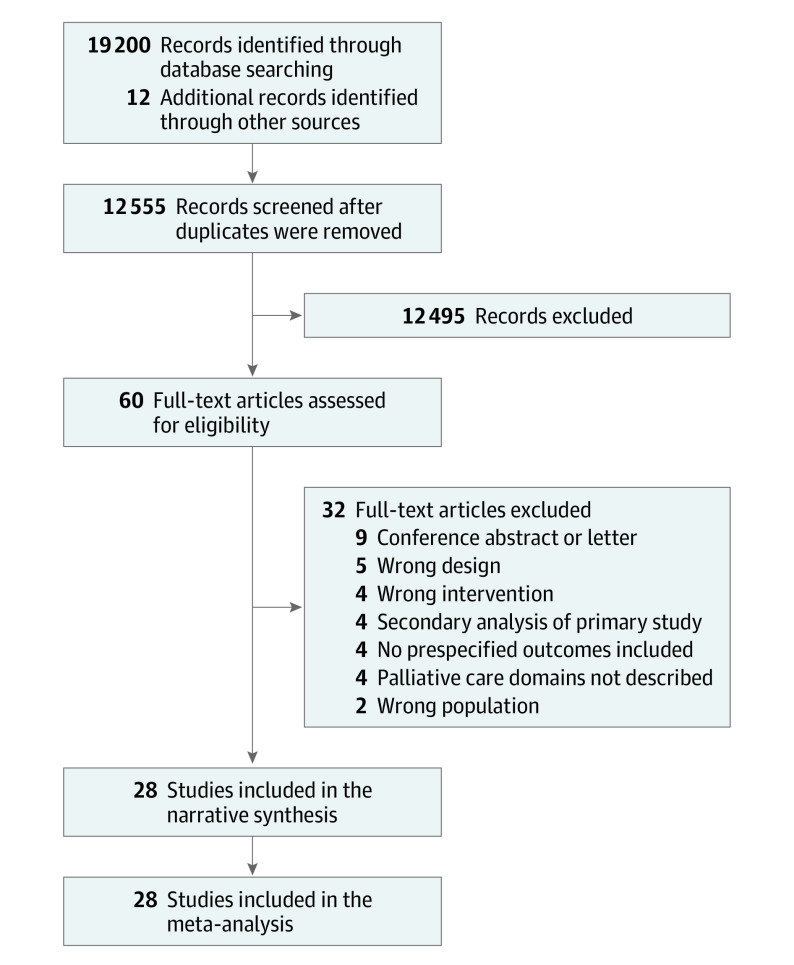
Data extraction and synthesis: Two reviewers independently screened, selected, and extracted data from studies. Narrative synthesis was conducted for all trials. All outcomes were analyzed using random-effects meta-analysis.
Main outcomes and measures: Acute health care use (hospitalizations and emergency department use), disease-generic and disease-specific quality of life (QOL), and symptoms, with estimates of QOL translated to units of the Functional Assessment of Chronic Illness Therapy-Palliative Care scale (range, 0 [worst] to 184 [best]; minimal clinically important difference, 9 points) and symptoms translated to units of the Edmonton Symptom Assessment Scale global distress score (range, 0 [best] to 90 [worst]; minimal clinically important difference, 5.7 points).
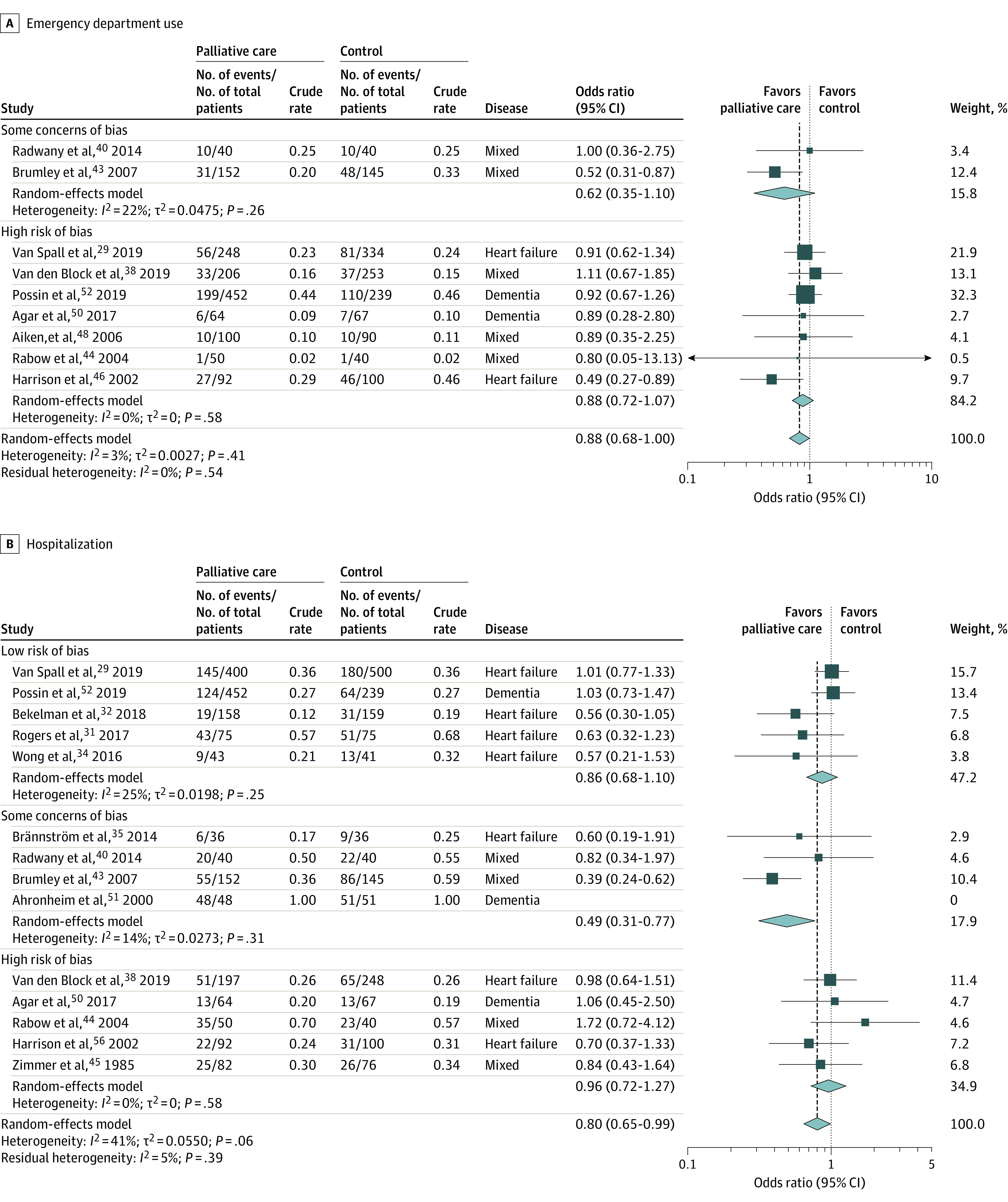
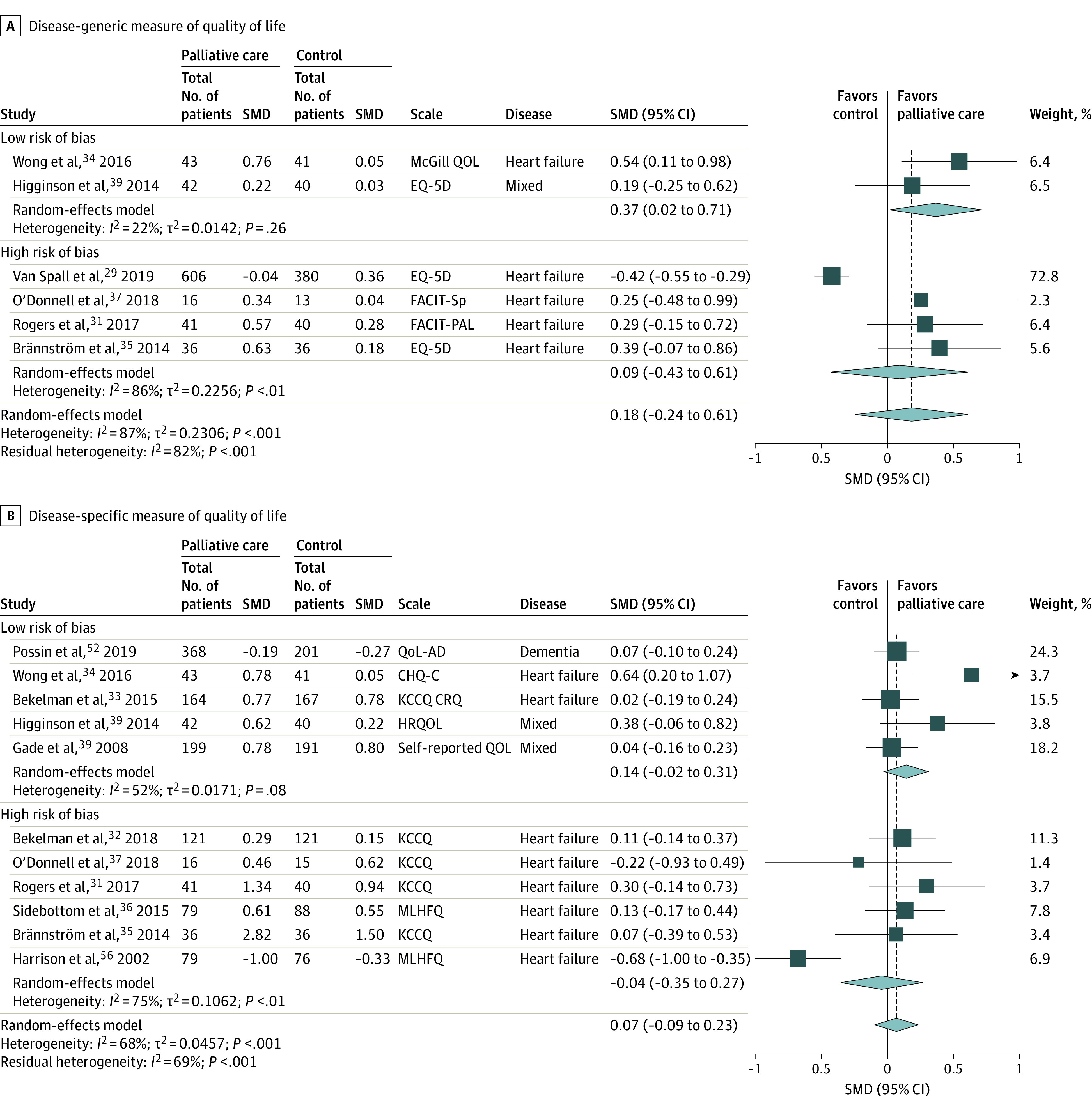
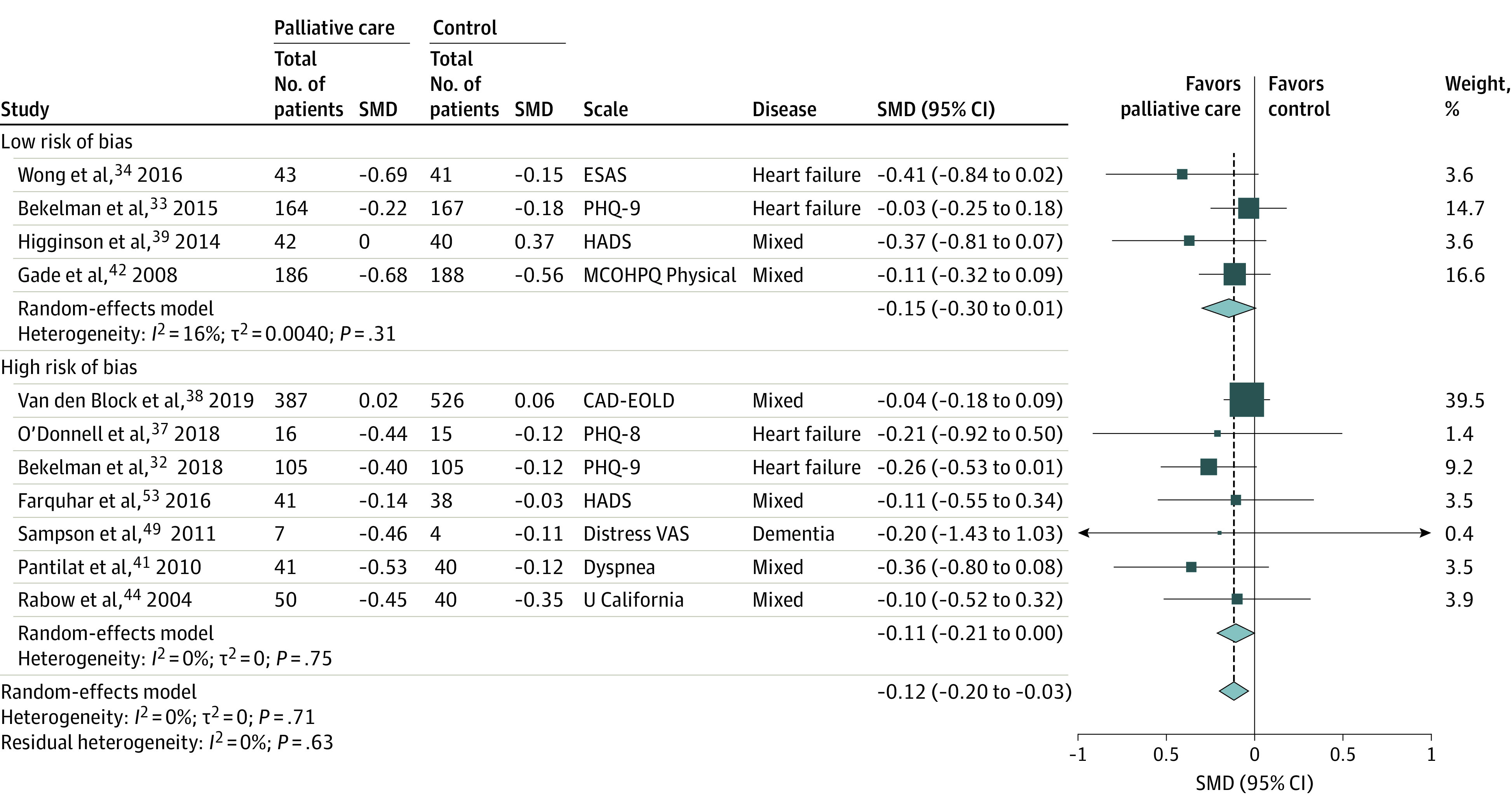
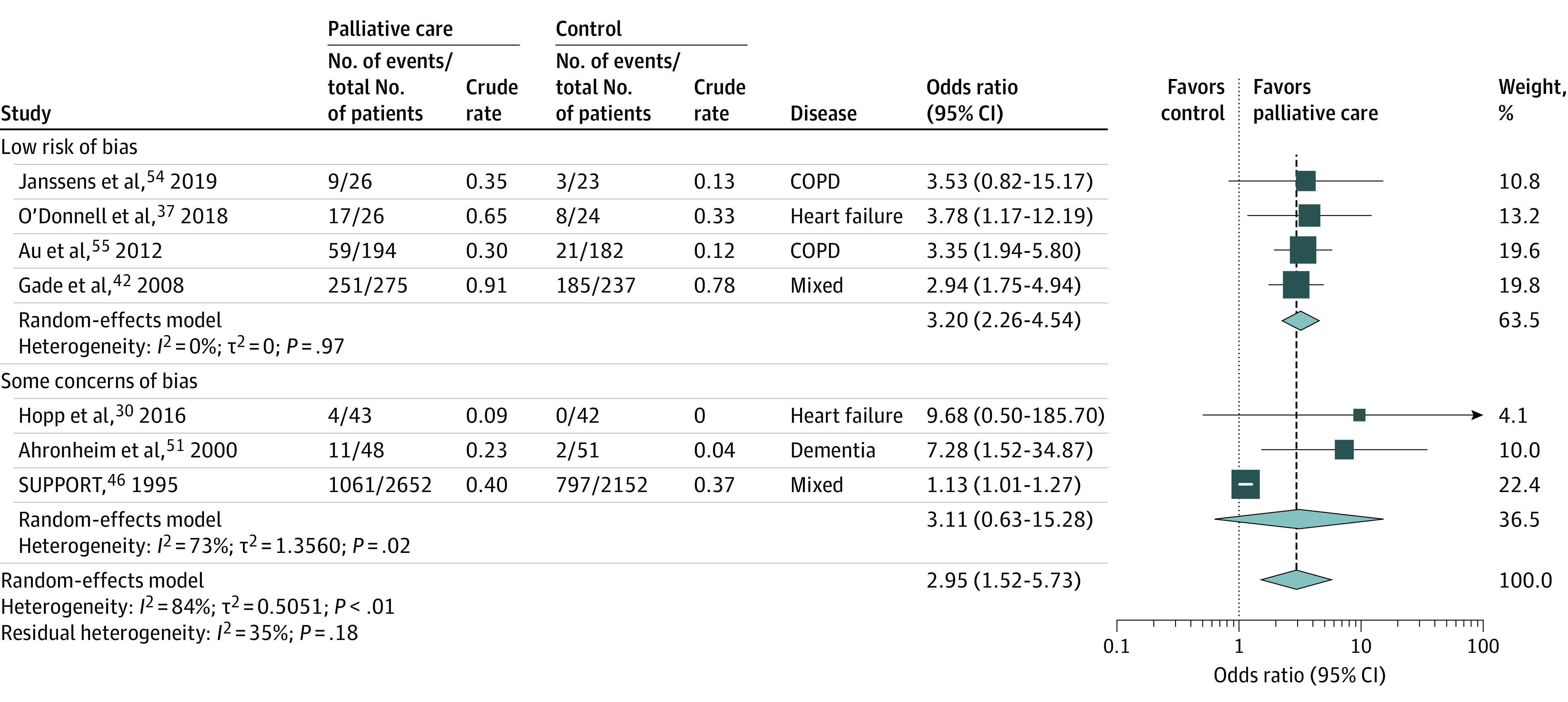
Results: Twenty-eight trials provided data on 13 664 patients (mean age, 74 years; 46% were women). Ten trials were of heart failure (n = 4068 patients), 11 of mixed disease (n = 8119), 4 of dementia (n = 1036), and 3 of chronic obstructive pulmonary disease (n = 441). Palliative care, compared with usual care, was statistically significantly associated with less emergency department use (9 trials [n = 2712]; 20% vs 24%; odds ratio, 0.82 [95% CI, 0.68-1.00]; I2 = 3%), less hospitalization (14 trials [n = 3706]; 38% vs 42%; odds ratio, 0.80 [95% CI, 0.65-0.99]; I2 = 41%), and modestly lower symptom burden (11 trials [n = 2598]; pooled standardized mean difference (SMD), -0.12; [95% CI, -0.20 to -0.03]; I2 = 0%; Edmonton Symptom Assessment Scale score mean difference, -1.6 [95% CI, -2.6 to -0.4]). Palliative care was not significantly associated with disease-generic QOL (6 trials [n = 1334]; SMD, 0.18 [95% CI, -0.24 to 0.61]; I2 = 87%; Functional Assessment of Chronic Illness Therapy-Palliative Care score mean difference, 4.7 [95% CI, -6.3 to 15.9]) or disease-specific measures of QOL (11 trials [n = 2204]; SMD, 0.07 [95% CI, -0.09 to 0.23]; I2 = 68%).
Conclusions and relevance: In this systematic review and meta-analysis of randomized clinical trials of patients with primarily noncancer illness, palliative care, compared with usual care, was statistically significantly associated with less acute health care use and modestly lower symptom burden, but there was no significant difference in quality of life. Analyses for some outcomes were based predominantly on studies of patients with heart failure, which may limit generalizability to other chronic illnesses.
Conflict of interest statement
Figures
Comment in
-
Palliative Care for Patients With Noncancer Illnesses.JAMA. 2020 Oct 13;324(14):1404-1405. doi: 10.1001/jama.2020.15075. JAMA. 2020. PMID: 33048142 Free PMC article. No abstract available.
-
In chronic noncancer illness, palliative care reduces symptoms and health care use but does not improve QoL.Ann Intern Med. 2021 Mar;174(3):JC31. doi: 10.7326/ACPJ202103160-031. Epub 2021 Mar 2. Ann Intern Med. 2021. PMID: 33646840
References
-
- Dementia numbers in Canada. Alzheimer Society Canada . Updated March 7, 2019. Accessed September 8, 2020. https://www.alzheimer.ca/en/About-dementia/What-is-dementia/Dementia-num...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
