

Psychosis in Alzheimer's Disease
- PMID: 33048274
- PMCID: PMC7554014
- DOI: 10.1007/s11910-020-01074-y
Psychosis in Alzheimer's Disease
Abstract
Purpose of review: To review the incidence, treatment and genetics of psychosis in people with mild cognitive impairment (MCI) and Alzheimer's disease (AD).
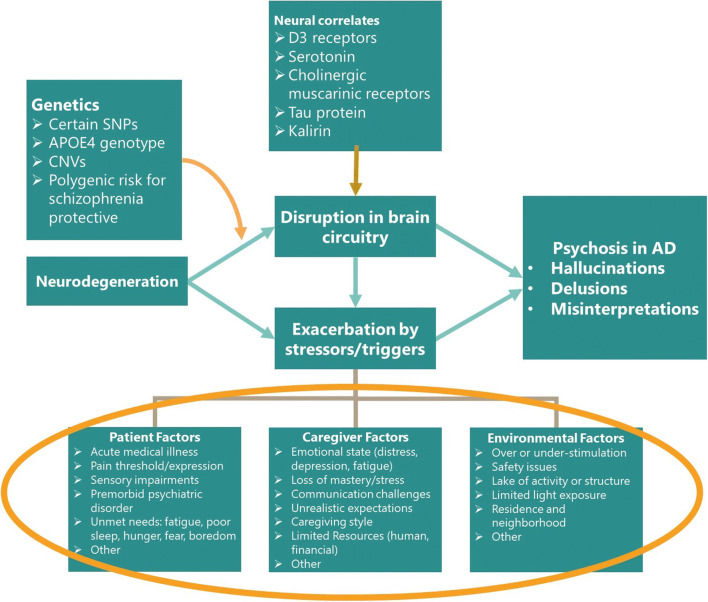
Recent findings: Psychosis in Alzheimer's disease (AD) has an incidence of ~ 10% per year. There is limited evidence regarding psychological interventions. Pharmacological management has focused on atypical antipsychotics, balancing modest benefits with evidence of long-term harms. The 5HT2A inverse agonist pimavanserin appears to confer benefit in PD psychosis with initial evidence of benefit in AD. Cholinesterase inhibitors give modest benefits in DLB psychosis. The utility of muscarinic agonists, lithium, glutamatergic and noradrenergic modulators needs further study. Recent work has confirmed the importance of psychosis in MCI as well as AD. The lack of evidence regarding psychological therapies is an urgent knowledge gap, but there is encouraging evidence for emerging pharmacological treatments. Genetics will provide an opportunity for precision medicine and new treatment targets.
Keywords: Alzheimer’s disease; Frequency; Impact; Mechanisms; Non-pharmacological; Pharmacological; Psychosis.
Conflict of interest statement
Prof Ballard reports grants from Biomedical Research Unit for Dementia (BRU-D) and the Maudsley Biomedical Research Centre (BRC)-dementia theme at the King’s College London, London, UK, during the conduct of the study; grants and personal fees from Acadia pharmaceutical company, grants and personal fees from Lundbeck, personal fees from Roche, personal fees from Otsuka, personal fees from Novartis, personal fees from Eli Lilly and personal fees from Pfizer, outside the submitted work. Prof Kales has royalties from the proceeds of the DICE Approach book. Prof Lyketsos wishes to acknowledge Johns Hopkins ADRC for supporting his time: P50AG005146. Prof Aarsland has received research support and/or honoraria from Astra-Zeneca, H. Lundbeck, Novartis Pharmaceuticals and GE Health and served as paid consultant for H. Lundbeck, Eisai, Heptares and Mentis Cura. Dag Aarsland is a Royal Society Wolfson Research Merit Award Holder and would like to thank the Wolfson Foundation and the Royal Society for their support. This paper represents independent research [part] funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. Dr Creese has no conflicts to disclose. Dr Mills reports other from Acadia Pharmaceuticals and personal fees from Addex Therapeutics, outside the submitted work. In addition, Dr Mills has a patent Mills R and Williams H., Patent PCT/US2013/071792: Methods for the treatment of Parkinson’s disease psychosis using pimavanserin; published 5 Jun 2014; pending. Dr Williams reports other from Acadia Pharmaceuticals and personal fees from Addex Pharmaceuticals, outside the submitted work; in addition, Dr Williams has a patent Mills R. and Williams H., Patent PCT/US2013/071792: Methods for the treatment of Parkinson’s disease psychosis using pimavanserin; published 5 Jun 2014, pending. Dr Sweet has nothing to disclose.
References
-
- Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, Ames D, Ballard C, Banerjee S, Burns A, Cohen-Mansfield J, Cooper C, Fox N, Gitlin LN, Howard R, Kales HC, Larson EB, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care. Lancet. 2017;390:2673–2734. - PubMed
-
- Haupt M, Kurz A, Janner M. A 2-year follow-up of behavioural and psychological symptoms in Alzheimer's disease. Dement Geriatr Cogn Disord. 2000;11:147–152. - PubMed
-
- Ballard C, Gray A, Ayre G. Psychotic symptoms, aggression and restlessness in dementia. Rev Neurol (Paris) 1999;155(Suppl 4):S44–S52. - PubMed
-
- Jeste DV, Finkel SI. Psychosis of Alzheimer’s disease and related dementias: diagnostic criteria for a distinct syndrome. Am J Geriatr Psychiatry. 2000;8:29–34. - PubMed
-
- Leroi I, Voulgari A, Breitner JC, et al. The epidemiology of psychosis in dementia. Am J Geriatr Psychiatry. 2003;11:83–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
