

Frequency and Clinical Utility of Olfactory Dysfunction in COVID-19: a Systematic Review and Meta-analysis
- PMID: 33048282
- PMCID: PMC7552599
- DOI: 10.1007/s11882-020-00972-y
Frequency and Clinical Utility of Olfactory Dysfunction in COVID-19: a Systematic Review and Meta-analysis
Abstract
Background: Olfactory dysfunction (OD) has been gaining recognition as a symptom of COVID-19, but its clinical utility has not been well defined.
Objectives: To quantify the clinical utility of identifying OD in the diagnosis of COVID-19 and determine an estimate of the frequency of OD amongst these patients.
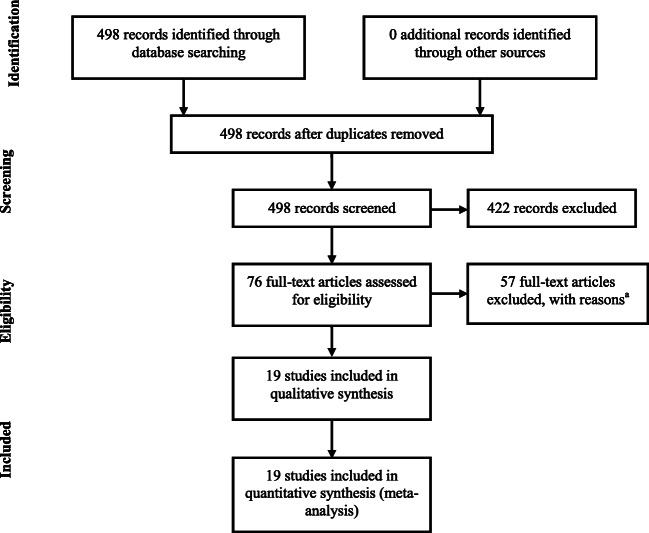
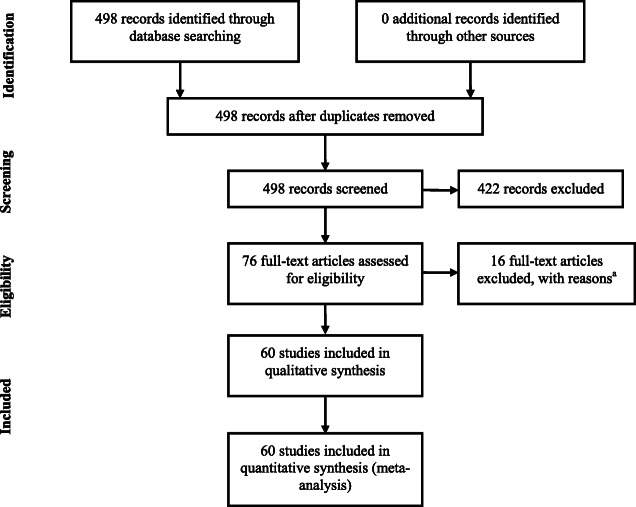
Methods: PubMed was searched up to 1 August 2020. Meta-analysis A included studies if they compared the frequency of OD in COVID-19 positive patients (proven by reverse transcription polymerase chain reaction) to COVID-19 negative controls. Meta-analysis B included studies if they described the frequency of OD in COVID-19 positive patients and if OD symptoms were explicitly asked in questionnaires or interviews or if smell tests were performed.
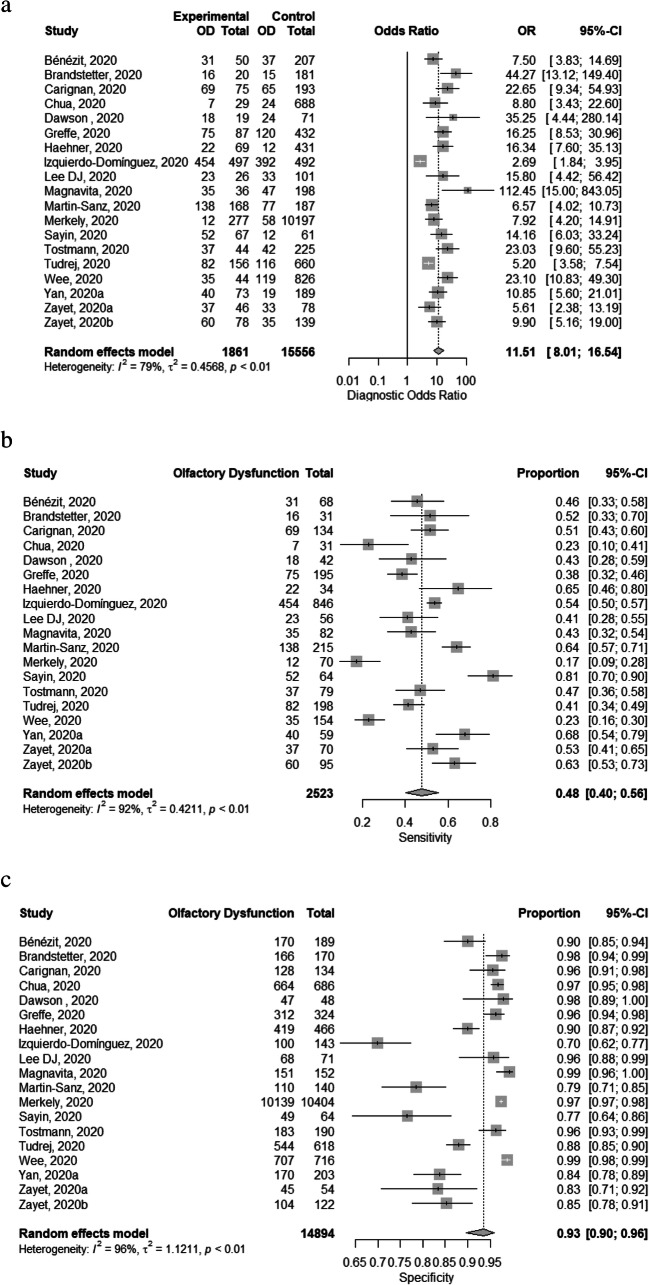
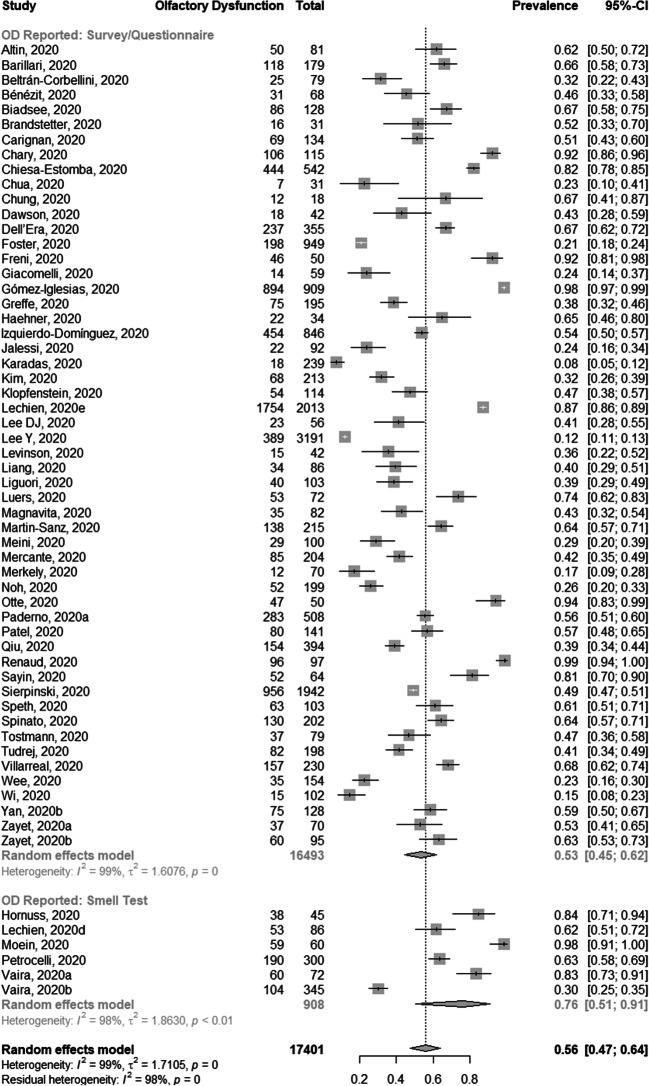
Results: The pooled frequency of OD in COVID-19 positive patients (17,401 patients, 60 studies) was 0.56 (0.47-0.64) but differs between detection via smell testing (0.76 [0.51-0.91]) and survey/questionnaire report (0.53 [0.45-0.62]), although not reaching statistical significance (p = 0.089). Patients with reported OD were more likely to test positive for COVID-19 (diagnostic odds ratio 11.5 [8.01-16.5], sensitivity 0.48 (0.40 to 0.56), specificity 0.93 (0.90 to 0.96), positive likelihood ratio 6.10 (4.47-8.32) and negative likelihood ratio 0.58 (0.52-0.64)). There was significant heterogeneity amongst studies with possible publication bias.
Conclusion: Frequency of OD in COVID-19 differs greatly across studies. Nevertheless, patients with reported OD were significantly more likely to test positive for COVID-19. Patient-reported OD is a highly specific symptom of COVID-19 which should be included as part of the pre-test screening of suspect patients.
Keywords: COVID-19; Coronavirus 2; Meta-analysis; Olfaction disorders; Severe acute respiratory syndrome.
Conflict of interest statement
The authors declare no conflicts of interest relevant to this manuscript.
Figures

References
-
- Izquierdo-Dominguez A, Rojas-Lechuga MJ, Mullol J, Alobid I. Olfactory dysfunction in the COVID-19 outbreak. J Investig Allergol Clin Immunol. 2020:0. 10.18176/jiaci.0567. - PubMed
-
- Mullol J, Alobid I, Mariño-Sánchez F, Quintó L, de Haro J, Bernal-Sprekelsen M, Valero A, Picado C, Marin C. Furthering the understanding of olfaction, prevalence of loss of smell and risk factors: a population-based survey (OLFACAT study) BMJ Open. 2012;2(6):e001256. doi: 10.1136/bmjopen-2012-001256. - DOI - PMC - PubMed
-
- ENT-UK. Loss of sense of smell as marker of COVID-19 infection. 2020. https://www.entuk.org/sites/default/files/files/Loss-of-sense-of-smell-0.... Accessed 9 May 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
