

The potential health impact of restricting less-healthy food and beverage advertising on UK television between 05.30 and 21.00 hours: A modelling study
- PMID: 33048922
- PMCID: PMC7553286
- DOI: 10.1371/journal.pmed.1003212
The potential health impact of restricting less-healthy food and beverage advertising on UK television between 05.30 and 21.00 hours: A modelling study
Abstract
Background: Restrictions on the advertising of less-healthy foods and beverages is seen as one measure to tackle childhood obesity and is under active consideration by the UK government. Whilst evidence increasingly links this advertising to excess calorie intake, understanding of the potential impact of advertising restrictions on population health is limited.
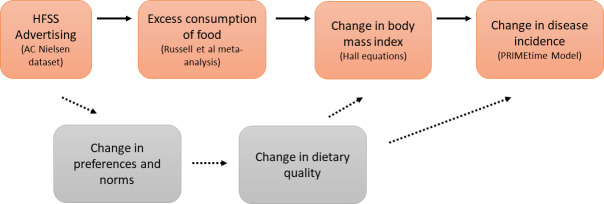
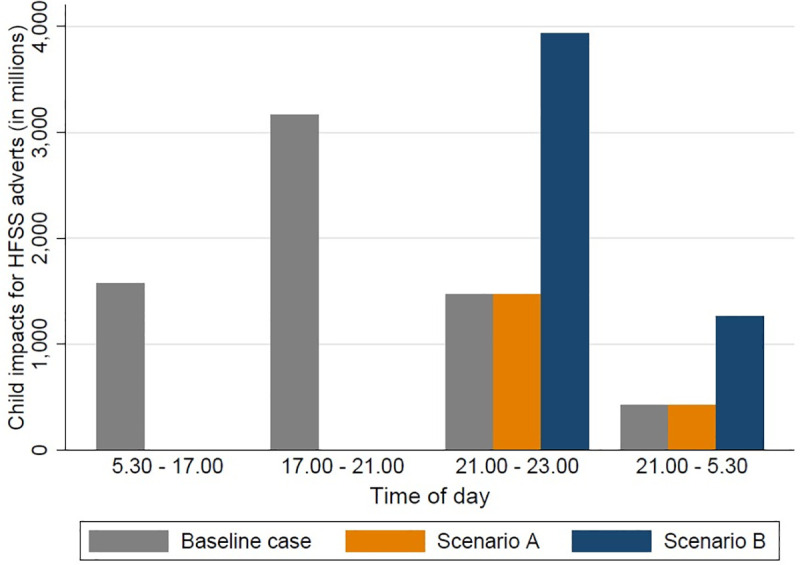
Methods and findings: We used a proportional multi-state life table model to estimate the health impact of prohibiting the advertising of food and beverages high in fat, sugar, and salt (HFSS) from 05.30 hours to 21.00 hours (5:30 AM to 9:00 PM) on television in the UK. We used the following data to parameterise the model: children's exposure to HFSS advertising from AC Nielsen and Broadcasters' Audience Research Board (2015); effect of less-healthy food advertising on acute caloric intake in children from a published meta-analysis; population numbers and all-cause mortality rates from the Human Mortality Database for the UK (2015); body mass index distribution from the Health Survey for England (2016); disability weights for estimating disability-adjusted life years (DALYs) from the Global Burden of Disease Study; and healthcare costs from NHS England programme budgeting data. The main outcome measures were change in the percentage of the children (aged 5-17 years) with obesity defined using the International Obesity Task Force cut-points, and change in health status (DALYs). Monte Carlo analyses was used to estimate 95% uncertainty intervals (UIs). We estimate that if all HFSS advertising between 05.30 hours and 21.00 hours was withdrawn, UK children (n = 13,729,000), would see on average 1.5 fewer HFSS adverts per day and decrease caloric intake by 9.1 kcal (95% UI 0.5-17.7 kcal), which would reduce the number of children (aged 5-17 years) with obesity by 4.6% (95% UI 1.4%-9.5%) and with overweight (including obesity) by 3.6% (95% UI 1.1%-7.4%) This is equivalent to 40,000 (95% UI 12,000-81,000) fewer UK children with obesity, and 120,000 (95% UI 34,000-240,000) fewer with overweight. For children alive in 2015 (n = 13,729,000), this would avert 240,000 (95% UI 65,000-530,000) DALYs across their lifetime (i.e., followed from 2015 through to death), and result in a health-related net monetary benefit of £7.4 billion (95% UI £2.0 billion-£16 billion) to society. Under a scenario where all HFSS advertising is displaced to after 21.00 hours, rather than withdrawn, we estimate that the benefits would be reduced by around two-thirds. This is a modelling study and subject to uncertainty; we cannot fully and accurately account for all of the factors that would affect the impact of this policy if implemented. Whilst randomised trials show that children exposed to less-healthy food advertising consume more calories, there is uncertainty about the nature of the dose-response relationship between HFSS advertising and calorie intake.
Conclusions: Our results show that HFSS television advertising restrictions between 05.30 hours and 21.00 hours in the UK could make a meaningful contribution to reducing childhood obesity. We estimate that the impact on childhood obesity of this policy may be reduced by around two-thirds if adverts are displaced to after 21.00 hours rather than being withdrawn.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RV MO RS KS report a grant for the Obesity Policy Research Unit, funded through the National Institute for Health Research (NIHR) to inform the work of the Department for Health and Social Care; OM was an advisor to the Health Select Committee during their inquiry into childhood obesity (2017-18).
Figures
References
-
- Lobstein T, Brinsden HC. Atlas of childhood obesity. London: World Obesity Federation; 2019. [cited 2020 Sep 15]. Available from:http://s3-eu-west-1.amazonaws.com/wof-files/11996_Childhood_Obesity_Atla....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
