

Universal third-trimester ultrasonic screening using fetal macrosomia in the prediction of adverse perinatal outcome: A systematic review and meta-analysis of diagnostic test accuracy
- PMID: 33048935
- PMCID: PMC7553291
- DOI: 10.1371/journal.pmed.1003190
Universal third-trimester ultrasonic screening using fetal macrosomia in the prediction of adverse perinatal outcome: A systematic review and meta-analysis of diagnostic test accuracy
Abstract
Background: The effectiveness of screening for macrosomia is not well established. One of the critical elements of an effective screening program is the diagnostic accuracy of a test at predicting the condition. The objective of this study is to investigate the diagnostic effectiveness of universal ultrasonic fetal biometry in predicting the delivery of a macrosomic infant, shoulder dystocia, and associated neonatal morbidity in low- and mixed-risk populations.
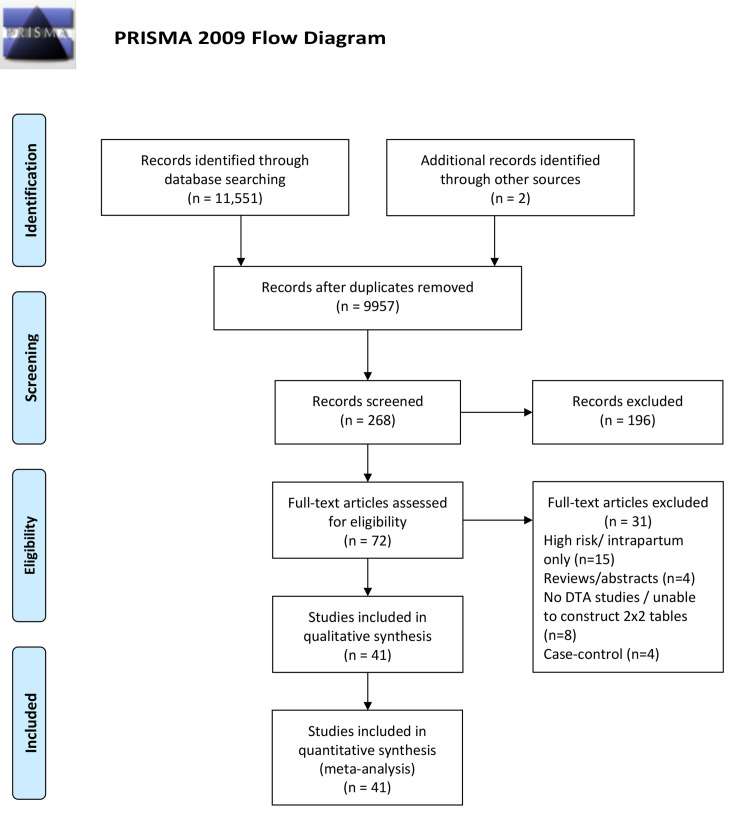
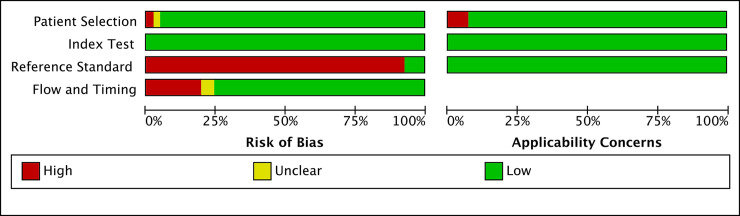
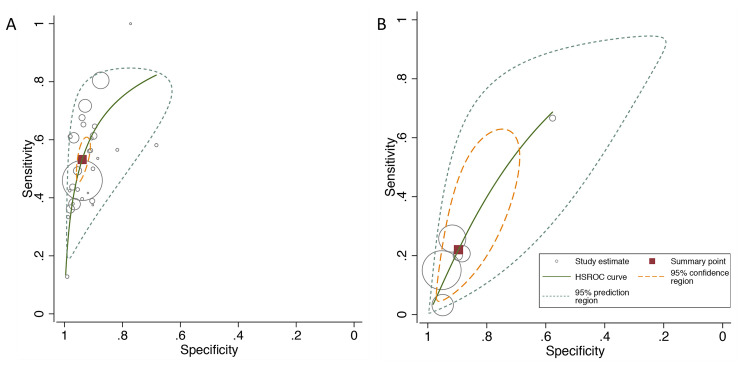
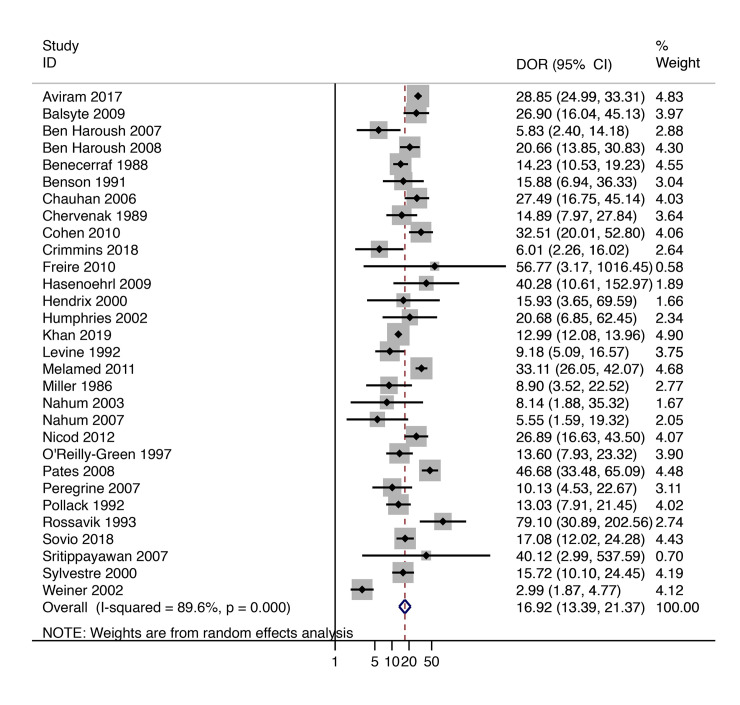
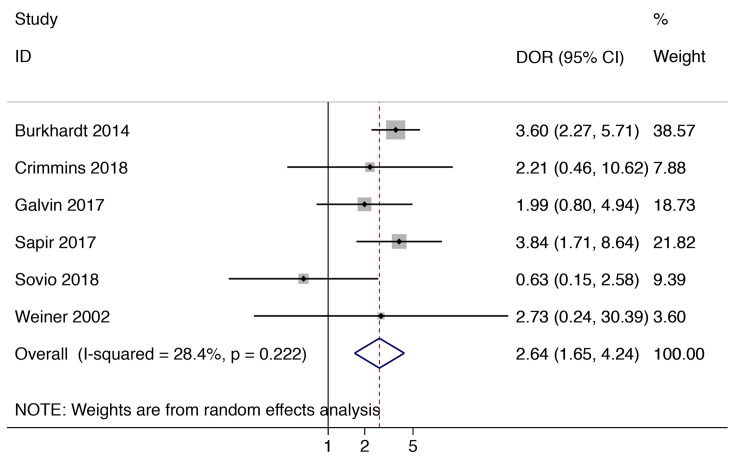
Methods and findings: We conducted a predefined literature search in Medline, Excerpta Medica database (EMBASE), the Cochrane library and ClinicalTrials.gov from inception to May 2020. No language restrictions were applied. We included studies where the ultrasound was performed as part of universal screening and those that included low- and mixed-risk pregnancies and excluded studies confined to high risk pregnancies. We used the estimated fetal weight (EFW) (multiple formulas and thresholds) and the abdominal circumference (AC) to define suspected large for gestational age (LGA). Adverse perinatal outcomes included macrosomia (multiple thresholds), shoulder dystocia, and other markers of neonatal morbidity. The risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool. Meta-analysis was carried out using the hierarchical summary receiver operating characteristic (ROC) and the bivariate logit-normal (Reitsma) models. We identified 41 studies that met our inclusion criteria involving 112,034 patients in total. These included 11 prospective cohort studies (N = 9986), one randomized controlled trial (RCT) (N = 367), and 29 retrospective cohort studies (N = 101,681). The quality of the studies was variable, and only three studies blinded the ultrasound findings to the clinicians. Both EFW >4,000 g (or 90th centile for the gestational age) and AC >36 cm (or 90th centile) had >50% sensitivity for predicting macrosomia (birthweight above 4,000 g or 90th centile) at birth with positive likelihood ratios (LRs) of 8.74 (95% confidence interval [CI] 6.84-11.17) and 7.56 (95% CI 5.85-9.77), respectively. There was significant heterogeneity at predicting macrosomia, which could reflect the different study designs, the characteristics of the included populations, and differences in the formulas used. An EFW >4,000 g (or 90th centile) had 22% sensitivity at predicting shoulder dystocia with a positive likelihood ratio of 2.12 (95% CI 1.34-3.35). There was insufficient data to analyze other markers of neonatal morbidity.
Conclusions: In this study, we found that suspected LGA is strongly predictive of the risk of delivering a large infant in low- and mixed-risk populations. However, it is only weakly (albeit statistically significantly) predictive of the risk of shoulder dystocia. There was insufficient data to analyze other markers of neonatal morbidity.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: AAM, NS, PB, JGT, and SCR have no competing interests to declare. US reports grants from NIHR Cambridge Biomedical Research Centre during the conduct of the study. GCS is a member of the Editorial Board of PLOS Medicine. GCS reports grants and personal fees from GlaxoSmithKline Research and Development, Ltd., grants from Sera Prognostics, Inc., nonfinancial support from Illumina, Inc., and personal fees from Roche Diagnostics, Ltd., outside the submitted work. In addition, GCS and US have a patent in preparation for a novel predictive test for fetal size pending. AP reports personal fees from educational events/lectures, clinical services in the private sector and from Consultancy via Oxford University Innovation, royalties from published works, and editorial work for UOG and BJOG, outside the submitted work.
Figures
References
-
- Esakoff TF, Cheng YW, Sparks TN, Caughey AB. The association between birthweight 4000 g or greater and perinatal outcomes in patients with and without gestational diabetes mellitus. American journal of obstetrics and gynecology. 2009;200(6):672.e1–4. Epub 2009/04/21. 10.1016/j.ajog.2009.02.035 . - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
