

Association of supratotal resection with progression-free survival, malignant transformation, and overall survival in lower-grade gliomas
- PMID: 33049063
- PMCID: PMC8099476
- DOI: 10.1093/neuonc/noaa225
Association of supratotal resection with progression-free survival, malignant transformation, and overall survival in lower-grade gliomas
Abstract
Background: Supratotal resection is advocated in lower-grade gliomas (LGGs) based on theoretical advantages but with limited verification of functional risk and data on oncological outcomes. We assessed the association of supratotal resection in molecularly defined LGGs with oncological outcomes.
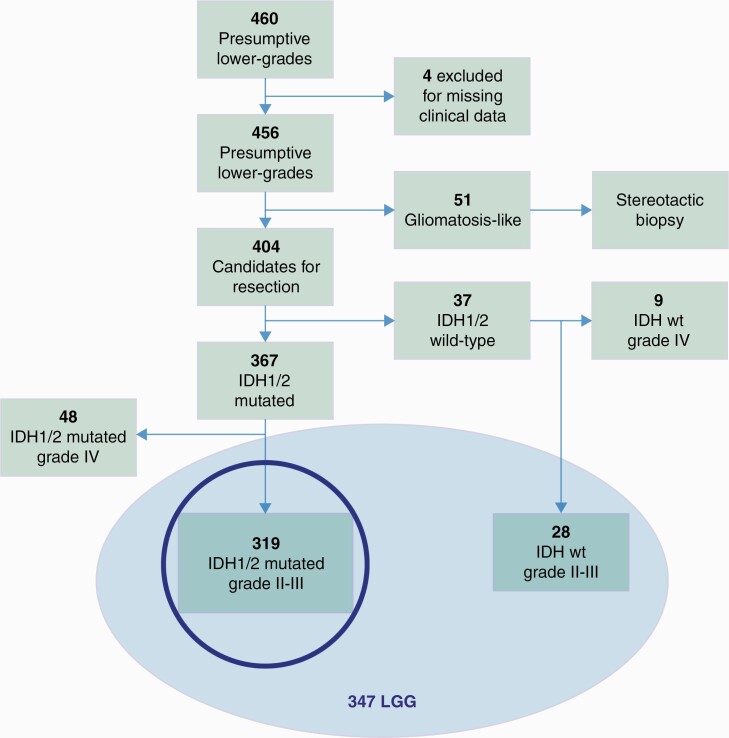
Methods: Included were 460 presumptive LGGs; 404 resected; 347 were LGGs, 319 isocitrate dehydrogenase (IDH)-mutated, 28 wildtype. All patients had clinical, imaging, and molecular data. Resection aimed at supratotal resection without any patient or tumor a priori selection. The association of extent of resection (EOR), categorized on volumetric fluid attenuated inversion recovery images as residual tumor volume, along with postsurgical management with progression-free survival (PFS), malignant (M)PFS, and overall survival (OS) assessed by univariate, multivariate, and propensity score analysis. The study mainly focused on IDH-mutated LGGs, the "typical LGGs."
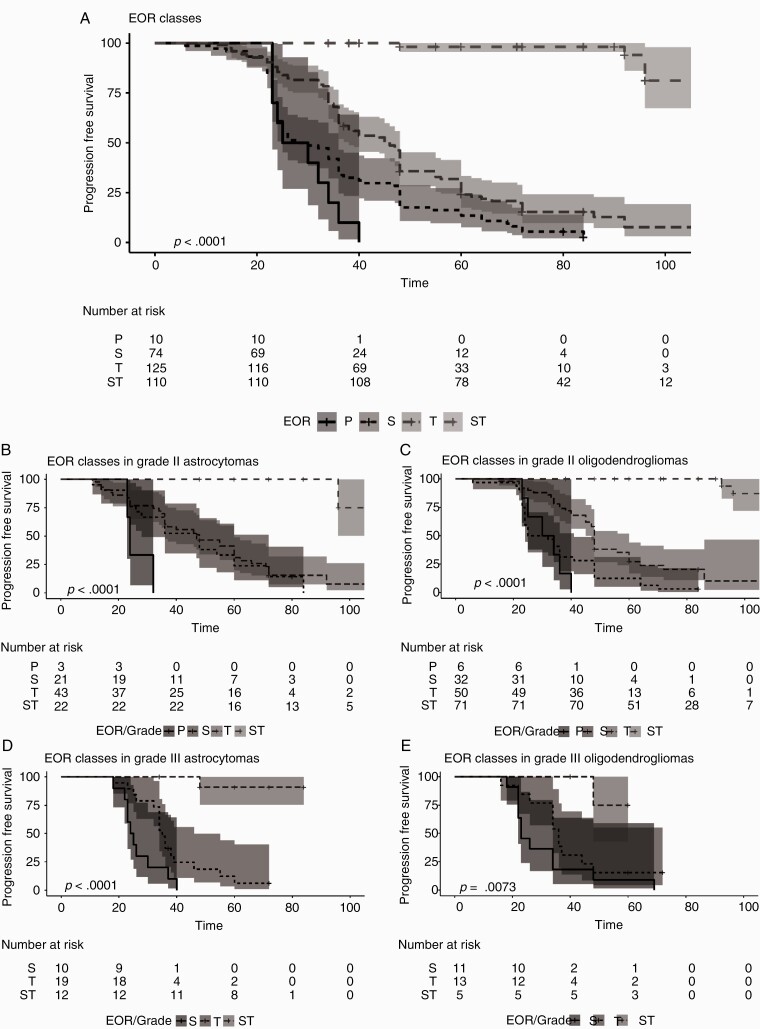
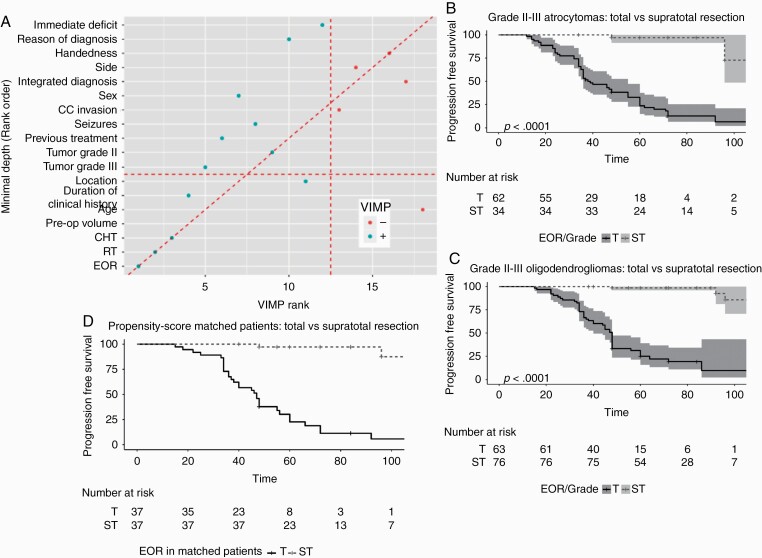
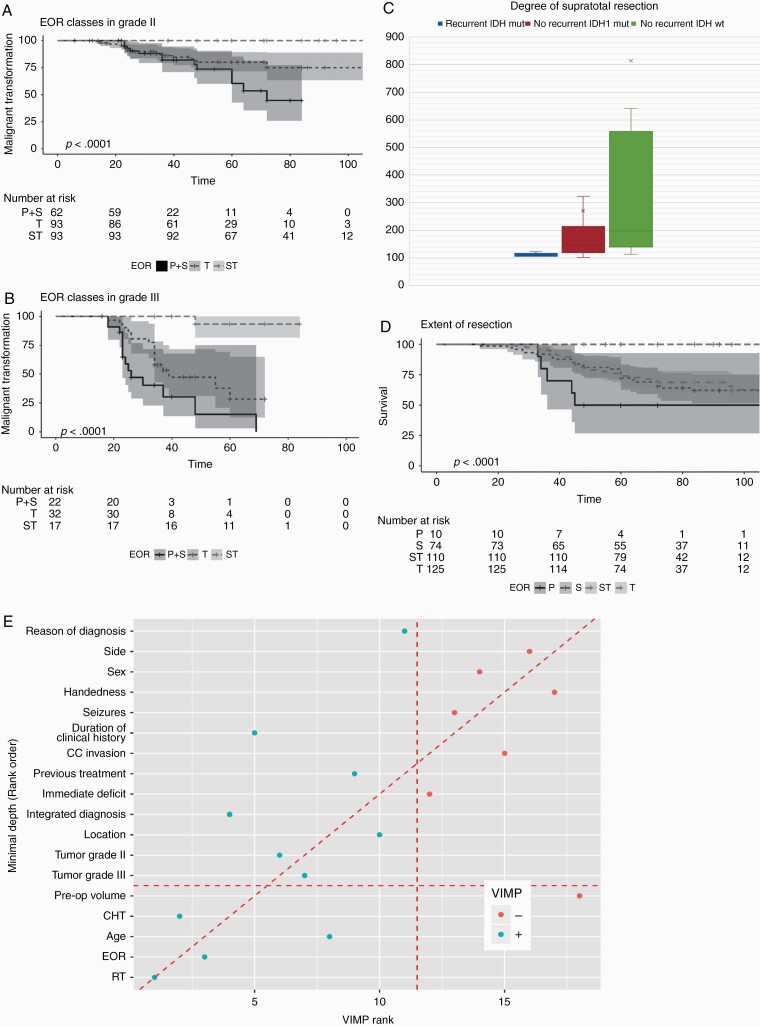
Results: Median follow-up was 6.8 years (interquartile range, 5-8). Out of 319 IDH-mutated LGGs, 190 (59.6%) progressed, median PFS: 4.7 years (95% CI: 4-5.3). Total and supratotal resection obtained in 39% and 35% of patients with IDH1-mutated tumors. In IDH-mutated tumors, most patients in the partial/subtotal group progressed, 82.4% in total, only 6 (5.4%) in supratotal. Median PFS was 29 months (95% CI: 25-36) in subtotal, 46 months (95% CI: 38-48) in total, while at 92 months, PFS in supratotal was 94.0%. There was no association with molecular subtypes and grade. At random forest analysis, PFS strongly associated with EOR, radiotherapy, and previous treatment. In the propensity score analysis, EOR associated with PFS (hazard ratio, 0.03; 95% CI: 0.01-0.13). MPFS occurred in 32.1% of subtotal total groups; 1 event in supratotal. EOR, grade III, previous treatment correlated to MPFS. At random forest analysis, OS associated with EOR as well.
Conclusions: Supratotal resection strongly associated with PFS, MPFS, and OS in LGGs, regardless of molecular subtypes and grade, right from the beginning of clinical presentation.
Keywords: lower-grade gliomas; malignant progression-free survival; overall survival; progression-free survival; supratotal resection.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Buckner J, Giannini C, Eckel-Passow J, et al. Management of diffuse low-grade gliomas in adults—use of molecular diagnostics. Nat Rev Neurol. 2017;13(6):340–351. - PubMed
-
- Jakola AS, Myrmel KS, Kloster R, et al. Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA. 2012;308(18):1881–1888. - PubMed
