

Treatment with Intravenous Methylprednisolone in Patients with Graves' Orbitopathy Significantly Affects Adrenal Function: Assessment of Serum, Salivary Cortisol and Serum Dehydroepiandrosterone Sulfate
- PMID: 33050327
- PMCID: PMC7601692
- DOI: 10.3390/jcm9103233
Treatment with Intravenous Methylprednisolone in Patients with Graves' Orbitopathy Significantly Affects Adrenal Function: Assessment of Serum, Salivary Cortisol and Serum Dehydroepiandrosterone Sulfate
Abstract
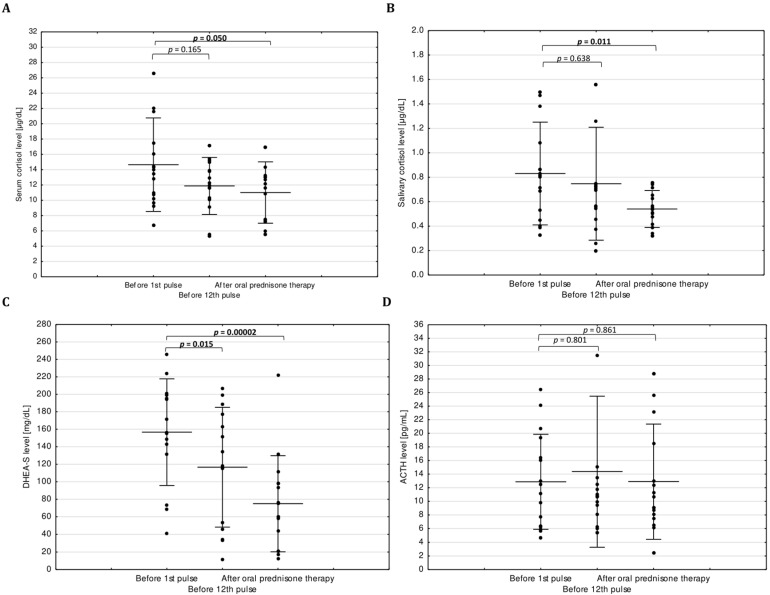
Treatment of active, moderate-to-severe Graves' orbitopathy (GO) is the administration of intravenous methylprednisolone (IVMP). IVMP may be followed by additional therapy with oral prednisone. The aim of this study was to analyze the impact of IVMP on adrenal function by evaluation of serum, salivary cortisol and serum dehydroepiandrosterone sulfate (DHEA-S). Fourteen patients received IVMP treatment (cumulative dose of 4.5 g in 12 weekly infusions) followed by oral prednisone (for three months). All patients showed normal adrenal function before the 12th IVMP pulse and one patient was diagnosed with secondary adrenal insufficiency (AI) after prednisone treatment. DHEA-S was significantly lower before the 12th IVMP pulse and after oral prednisone (p = 0.015 and p = 0.00002, respectively) in comparison to evaluation before therapy. DHEA-S levels were below the reference range in one and three patients before the 12th IVMP pulse and after prednisone therapy, respectively. We observed decreased serum (p = 0.05) and salivary (p = 0.011) cortisol levels after oral prednisone therapy in comparison to evaluation before therapy. Treatment with IVMP in a cumulative dose of 4.5 g affects adrenal function, causing more severe impairment of DHEA-S secretion than that of cortisol but does not cause secondary AI. Additional therapy with oral glucocorticoids after IVMP can cause secondary AI.
Keywords: Graves’ ophthalmopathy; Graves’ orbitopathy; adrenal insufficiency; dehydroepiandrosterone sulfate; glucocorticoids; methylprednisolone; salivary cortisol; serum cortisol.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bartalena L., Baldeschi L., Boboridis K., Eckstein A., Kahaly G.J., Marcocci C., Perros P., Salvi M., Wiersinga W.M. The 2016 European Thyroid Association/European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy. Eur. Thyroid J. 2016;5:9–26. doi: 10.1159/000443828. - DOI - PMC - PubMed
-
- Bartalena L., Baldeschi L., Dickinson A., Eckstein A., Kendall-Taylor P., Marcocci C., Mourits M., Perros P., Boboridis K., Boschi A., et al. Consensus statement of the European Group on Graves’ orbitopathy (EUGOGO) on management of GO. Eur. J. Endocrinol. 2008;158:273–285. doi: 10.1530/EJE-07-0666. - DOI - PubMed
-
- Bornstein S.R., Allolio B., Arlt W., Barthel A., Don-wauchope A., Hammer G.D., Husebye E.S., Merke D.P., Murad H., Stratakis C.A., et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016;101:364–389. doi: 10.1210/jc.2015-1710. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
