

Challenges in the Transition from In-Patient to Out-Patient Treatment in Depression
- PMID: 33050996
- PMCID: PMC7575898
- DOI: 10.3238/arztebl.2020.0472
Challenges in the Transition from In-Patient to Out-Patient Treatment in Depression
Abstract
Background: Few data are available on the characteristics of inpatient treatment and subsequent outpatient treatment for depression in Germany. In this study, we aimed to characterize the inpatient and outpatient treatment phases, to determine the rates of readmission and mortality, and to identify risk factors.
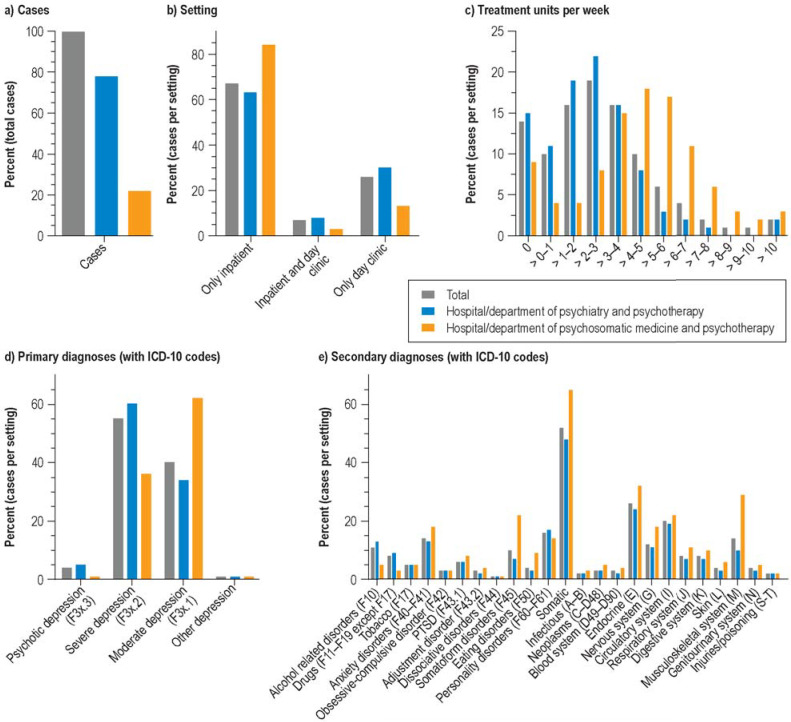
Methods: We carried out a descriptive statistical analysis of routine administrative data from a large health-insurance carrier (BARMER). All insurees aged 18 to 65 who were treated in 2015 as inpatients on a psychiatry and psychotherapy service or on a psychosomatic medicine and psychotherapy service with a main diagnosis of depression were included in the analysis. Risk factors for readmission and death were determined with the aid of mixed logistic regression.
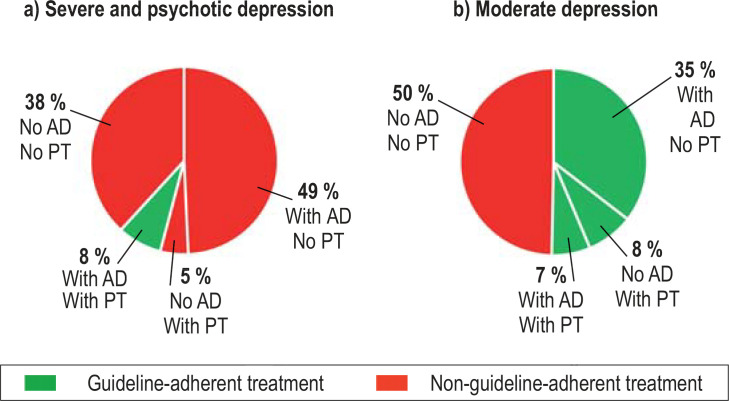
Results: Of the 22 893 patients whose data were analyzed, 78% had been hospitalized on a psychiatry and psychotherapy service and 22% on a psychosomatic medicine and psychotherapy service. The median length of hospital stay was 42 days. Follow-up care in the outpatient setting failed to conform with the recommendations of the pertinent guidelines in 92% of the patients with a main diagnosis of severe depression during hospitalization, and in 50% of those with moderate depression. 21% of the patients were readmitted within a year. The mortality at one year was 961 per 100 000 individuals (adjusted for the age and sex structure of the German population), or 3.4 times the mortality of the population at large. In the regression model, more treatment units during hospitalization and subsequent treatment with psychotherapy were associated with a lower probability of readmission, while longer hospitalization with subsequent pharmacotherapy or psychotherapy was associated with lower mortality.
Conclusion: The recommendations of the national (German) S3 guidelines for the further care of patients who have been hospitalized for depression are inadequately implemented at present in the sectored structures of in- and outpatient care in the German health care system. This patient group has marked excess mortality.
Figures
Comment in
-
Breaking Down Barriers in Outpatient Treatment.Dtsch Arztebl Int. 2021 Jan 29;118(4):57. doi: 10.3238/arztebl.m2021.0049. Dtsch Arztebl Int. 2021. PMID: 33759748 Free PMC article. No abstract available.
-
Alarming Figures for Severe and Moderate-to-Severe Depression.Dtsch Arztebl Int. 2021 Jan 29;118(4):57. doi: 10.3238/arztebl.m2021.0050. Dtsch Arztebl Int. 2021. PMID: 33759749 Free PMC article. No abstract available.
References
-
- Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3:171–178. - PubMed
-
- Melchior H, Schulz H, Härter M. Faktencheck Gesundheit. Bertelsmann Stiftung. 2014:1–144.
-
- Nordentoft M, Mortensen PB, Pedersen CB. Absolute risk of suicide after first hospital contact in mental disorder. Arch Gen Psychiatry. 2011;68:1058–1064. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical