

False Positive Multiparametric Magnetic Resonance Imaging Phenotypes in the Biopsy-naïve Prostate: Are They Distinct from Significant Cancer-associated Lesions? Lessons from PROMIS
- PMID: 33051065
- PMCID: PMC7772750
- DOI: 10.1016/j.eururo.2020.09.043
False Positive Multiparametric Magnetic Resonance Imaging Phenotypes in the Biopsy-naïve Prostate: Are They Distinct from Significant Cancer-associated Lesions? Lessons from PROMIS
Abstract
Background: False positive multiparametric magnetic resonance imaging (mpMRI) phenotypes prompt unnecessary biopsies. The Prostate MRI Imaging Study (PROMIS) provides a unique opportunity to explore such phenotypes in biopsy-naïve men with raised prostate-specific antigen (PSA) and suspected cancer.
Objective: To compare mpMRI lesions in men with/without significant cancer on transperineal mapping biopsy (TPM).
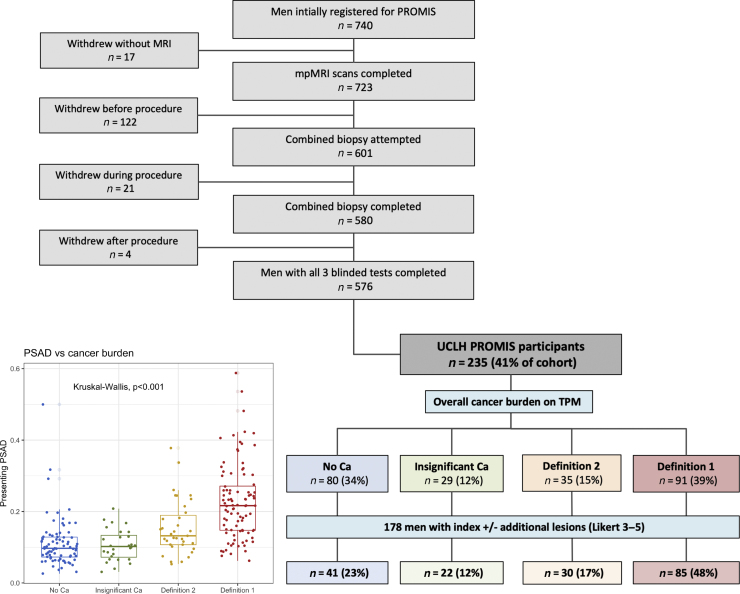
Design, setting, and participants: PROMIS participants (n=235) underwent mpMRI followed by a combined biopsy procedure at University College London Hospital, including 5-mm TPM as the reference standard. Patients were divided into four mutually exclusive groups according to TPM findings: (1) no cancer, (2) insignificant cancer, (3) definition 2 significant cancer (Gleason ≥3+4 of any length and/or maximum cancer core length ≥4mm of any grade), and (4) definition 1 significant cancer (Gleason ≥4+3 of any length and/or maximum cancer core length ≥6mm of any grade).
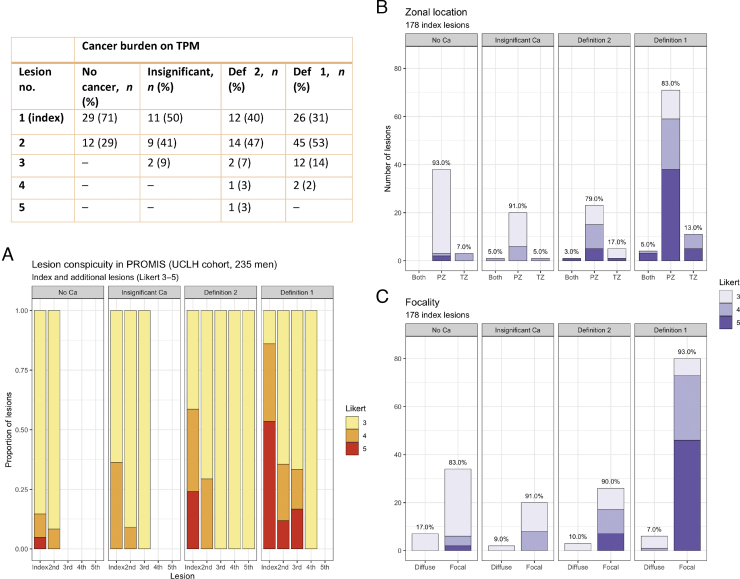
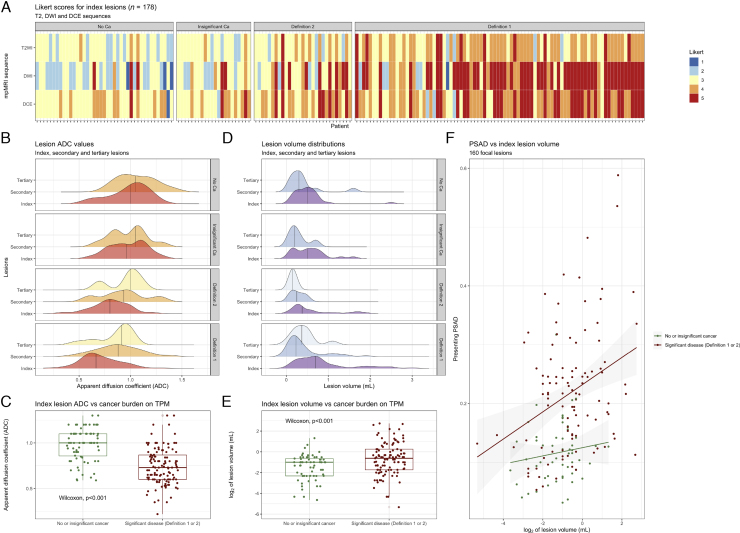
Outcome measurements and statistical analysis: Index and/or additional lesions present in 178 participants were compared between TPM groups in terms of number, conspicuity, volume, location, and radiological characteristics.
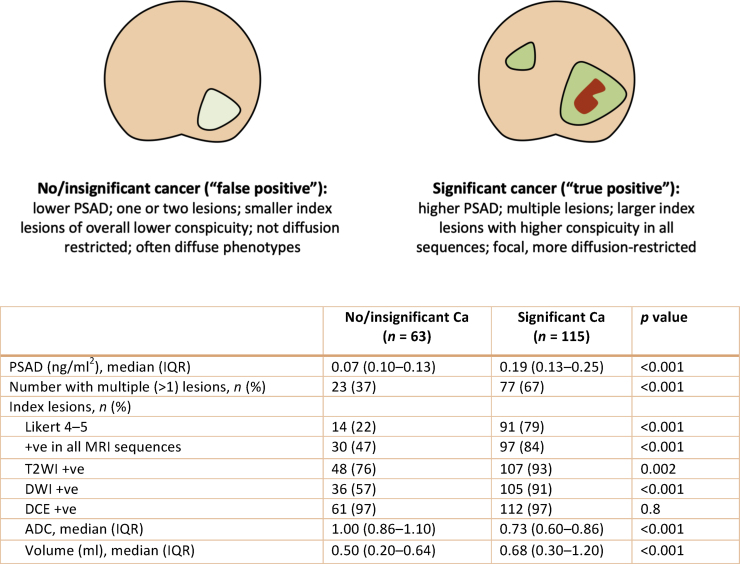
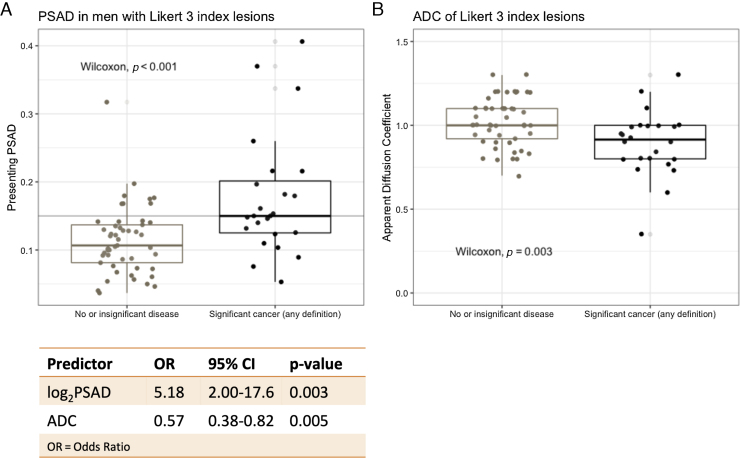
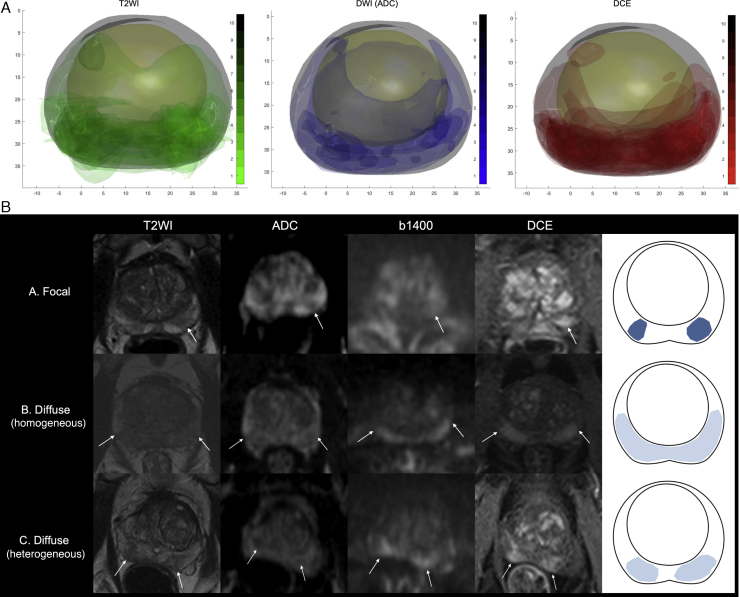
Results and limitations: Most lesions were located in the peripheral zone. More men with significant cancer had two or more lesions than those without significant disease (67% vs 37%; p< 0.001). In the former group, index lesions were larger (mean volume 0.68 vs 0.50 ml; p< 0.001, Wilcoxon test), more conspicuous (Likert 4-5: 79% vs 22%; p< 0.001), and diffusion restricted (mean apparent diffusion coefficient [ADC]: 0.73 vs 0.86; p< 0.001, Wilcoxon test). In men with Likert 3 index lesions, log2PSA density and index lesion ADC were significant predictors of definition 1/2 disease in a logistic regression model (mean cross-validated area under the receiver-operator characteristic curve: 0.77 [95% confidence interval: 0.67-0.87]).
Conclusions: Significant cancer-associated MRI lesions in biopsy-naïve men have clinical-radiological differences, with lesions seen in prostates without significant disease. MRI-calculated PSA density and ADC could predict significant cancer in those with indeterminate MRI phenotypes.
Patient summary: Magnetic resonance imaging (MRI) lesions that mimic prostate cancer but are, in fact, benign prompt unnecessary biopsies in thousands of men with raised prostate-specific antigen. In this study we found that, on closer look, such false positive lesions have different features from cancerous ones. This means that doctors could potentially develop better tools to identify cancer on MRI and spare some patients from unnecessary biopsies.
Keywords: False positive lesions; Multiparametric magnetic resonance imaging; PROMIS; Prostate cancer.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Restricting False-positive Magnetic Resonance Imaging Scans to Reduce Overdiagnosis of Prostate Cancer.Eur Urol. 2021 Jan;79(1):30-32. doi: 10.1016/j.eururo.2020.10.013. Epub 2020 Nov 6. Eur Urol. 2021. PMID: 33162247 No abstract available.
References
-
- National Institute for Health and Care Excellence (NICE). Guidance NG 131: prostate cancer diagnosis and management. https://www.nice.org.uk/guidance/ng131. - PubMed
-
- National Prostate Cancer Audit . 2019. National prostate Cancer audit annual report.https://www.npca.org.uk/reports/npca-annual-report-2019/
-
- Drost F.-J.H., Osses D., Nieboer D. Prostate magnetic resonance imaging, with or without magnetic resonance imaging-targeted biopsy, and systematic biopsy for detecting prostate cancer: a Cochrane systematic review and meta-analysis. Eur Urol. 2020;77:78–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
