

Cost-effectiveness of screening and treatment using direct-acting antivirals for chronic Hepatitis C virus in a primary care setting in Karachi, Pakistan
- PMID: 33051950
- PMCID: PMC7821258
- DOI: 10.1111/jvh.13422
Cost-effectiveness of screening and treatment using direct-acting antivirals for chronic Hepatitis C virus in a primary care setting in Karachi, Pakistan
Abstract
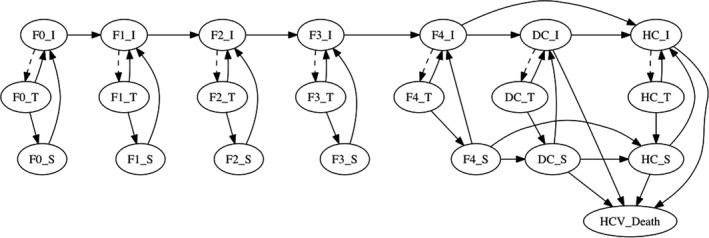
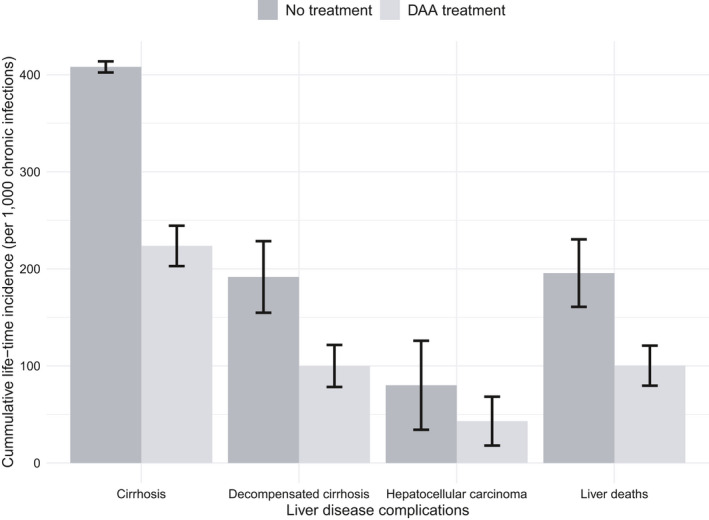
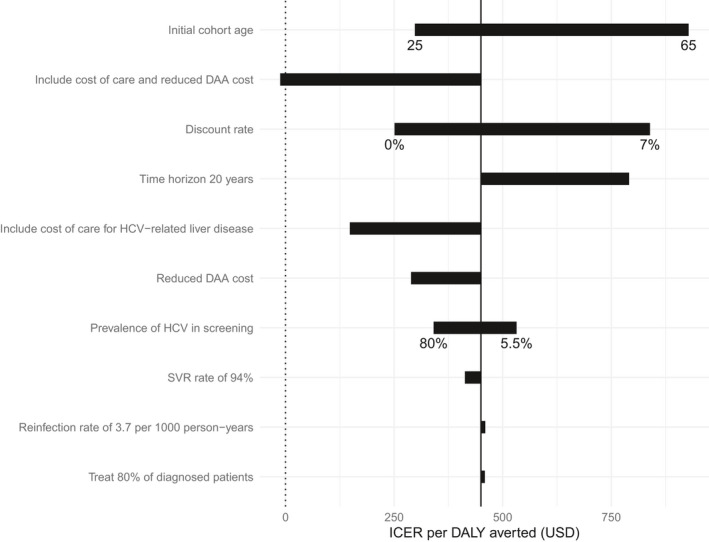
Despite the availability of effective direct-acting antiviral (DAA) treatments for Hepatitis C virus (HCV) infection, many people remain undiagnosed and untreated. We assessed the cost-effectiveness of a Médecins Sans Frontières (MSF) HCV screening and treatment programme within a primary health clinic in Karachi, Pakistan. A health state transition Markov model was developed to estimate the cost-effectiveness of the MSF programme. Programme cost and outcome data were analysed retrospectively. The incremental cost-effectiveness ratio (ICER) was calculated in terms of incremental cost (2016 US$) per disability-adjusted life year (DALY) averted from the provider's perspective over a lifetime horizon. The robustness of the model was evaluated using deterministic and probabilistic sensitivity analyses (PSA). The ICER for implementing testing and treatment compared to no programme was US$450/DALY averted, with 100% of PSA runs falling below the per capita Gross Domestic Product threshold for cost-effective interventions for Pakistan (US$1,422). The ICER increased to US$532/DALY averted assuming national HCV seroprevalence (5.5% versus 33% observed in the intervention). If the cost of liver disease care was included (adapted from resource use data from Cambodia which has similar GDP to Pakistan), the ICER dropped to US$148/DALY, while it became cost-saving if a recently negotiated reduced drug cost of $75/treatment course was assumed (versus $282 in base-case) in addition to cost of liver disease care. In conclusion, screening and DAA treatment for HCV infection are expected to be highly cost-effective in Pakistan, supporting the expansion of similar screening and treatment programmes across Pakistan.
Keywords: Pakistan; chronic hepatitis C; cost-effectiveness; low-income population; treatment costs.
© 2020 The Authors. Journal of Viral Hepatitis published by John Wiley & Sons Ltd.
Conflict of interest statement
PV has received unrestricted research grants from Gilead unrelated to this study and honoraria from Gilead and Abbvie. JGW has received a research grant from Gilead unrelated to this study. GGK, KA, YW, HZ, RVB, GF, RA, DD, CF and AL were employed by MSF and/or by Epicentre, an association created by MSF in 1986 to provide epidemiological expertise to underpin MSF operations. They participated in planning the study, carrying out the research and writing the report. The other authors declared no conflicts of interest.
Figures
References
-
- World Health Organisation . Global hepatitis report 2017. 2017: Geneva.
-
- Graham CS, Swan T. A path to eradication of hepatitis C in low‐ and middle‐income countries. Antiviral Res. 2015;119:89‐96. - PubMed
-
- Gower E, Estes C, Blach S, Razavi‐Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014;61(1 suppl):S45‐57. - PubMed
-
- Qureshi H, Bile KM, Jooma R, Alam SE, Afrid H. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. East Mediterr Health J. 2010;16(suppl):S15‐23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
