

A case-control and cohort study to determine the relationship between ethnic background and severe COVID-19
- PMID: 33052324
- PMCID: PMC7545271
- DOI: 10.1016/j.eclinm.2020.100574
A case-control and cohort study to determine the relationship between ethnic background and severe COVID-19
Abstract
Background: People of minority ethnic backgrounds may be disproportionately affected by severe COVID-19. Whether this relates to increased infection risk, more severe disease progression, or worse in-hospital survival is unknown. The contribution of comorbidities or socioeconomic deprivation to ethnic patterning of outcomes is also unclear.
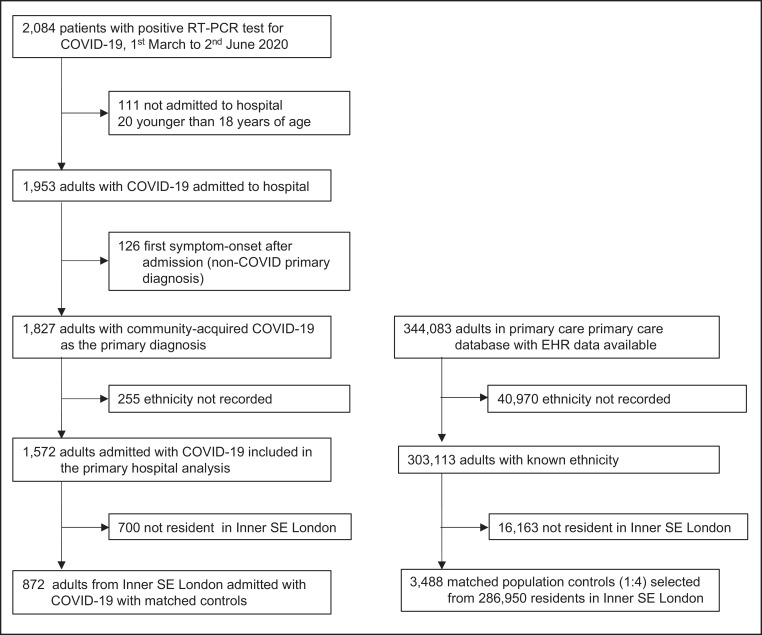
Methods: We conducted a case-control and a cohort study in an inner city primary and secondary care setting to examine whether ethnic background affects the risk of hospital admission with severe COVID-19 and/or in-hospital mortality. Inner city adult residents admitted to hospital with confirmed COVID-19 (n = 872 cases) were compared with 3,488 matched controls randomly sampled from a primary healthcare database comprising 344,083 people residing in the same region. For the cohort study, we studied 1827 adults consecutively admitted with COVID-19. The primary exposure variable was self-defined ethnicity. Analyses were adjusted for socio-demographic and clinical variables.
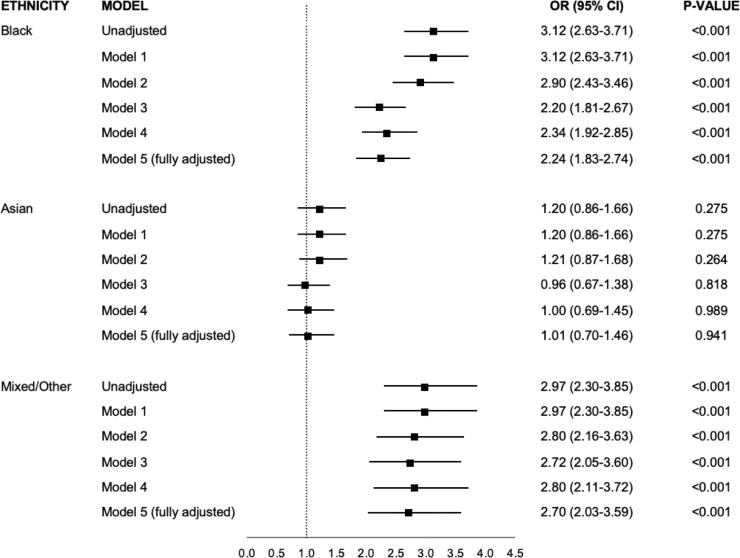
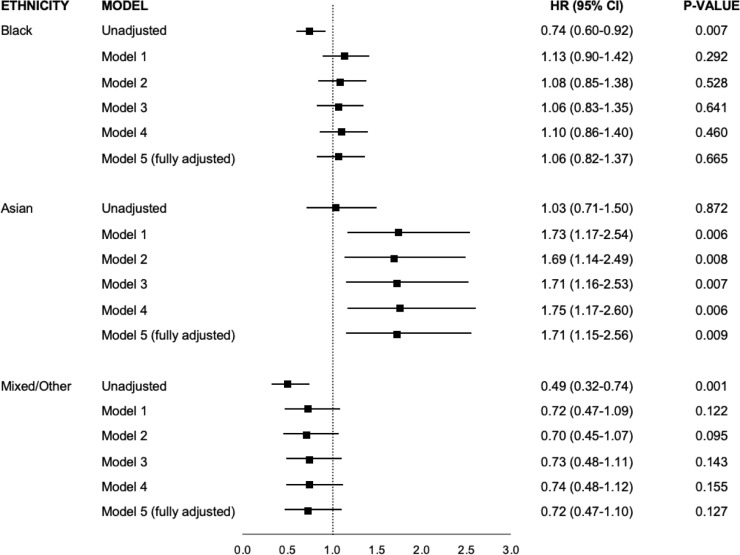
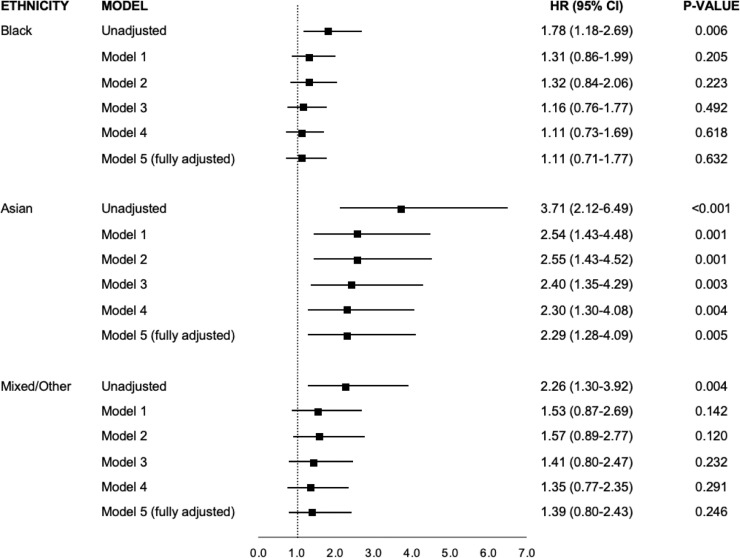
Findings: The 872 cases comprised 48.1% Black, 33.7% White, 12.6% Mixed/Other and 5.6% Asian patients. In conditional logistic regression analyses, Black and Mixed/Other ethnicity were associated with higher admission risk than white (OR 3.12 [95% CI 2.63-3.71] and 2.97 [2.30-3.85] respectively). Adjustment for comorbidities and deprivation modestly attenuated the association (OR 2.24 [1.83-2.74] for Black, 2.70 [2.03-3.59] for Mixed/Other). Asian ethnicity was not associated with higher admission risk (adjusted OR 1.01 [0.70-1.46]). In the cohort study of 1827 patients, 455 (28.9%) died over a median (IQR) of 8 (4-16) days. Age and male sex, but not Black (adjusted HR 1.06 [0.82-1.37]) or Mixed/Other ethnicity (adjusted HR 0.72 [0.47-1.10]), were associated with in-hospital mortality. Asian ethnicity was associated with higher in-hospital mortality but with a large confidence interval (adjusted HR 1.71 [1.15-2.56]).
Interpretation: Black and Mixed ethnicity are independently associated with greater admission risk with COVID-19 and may be risk factors for development of severe disease, but do not affect in-hospital mortality risk. Comorbidities and socioeconomic factors only partly account for this and additional ethnicity-related factors may play a large role. The impact of COVID-19 may be different in Asians.
Funding: British Heart Foundation; the National Institute for Health Research; Health Data Research UK.
Keywords: COVID-19; Case-control study; Comorbidities; Deprivation; Ethnicity.
© 2020 The Author(s).
Conflict of interest statement
JTHT received research funding from Innovate UK & Office of Life Sciences, and iRhythm Technologies, and holds shares <£5000 in Glaxo Smithkline and Biogen. The other authors declare no competing interests.
Figures
References
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323:1239–1242. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
