

Treatment variables associated with outcome in emergency department patients with suspected sepsis
- PMID: 33052499
- PMCID: PMC7560670
- DOI: 10.1186/s13613-020-00747-8
Treatment variables associated with outcome in emergency department patients with suspected sepsis
Abstract
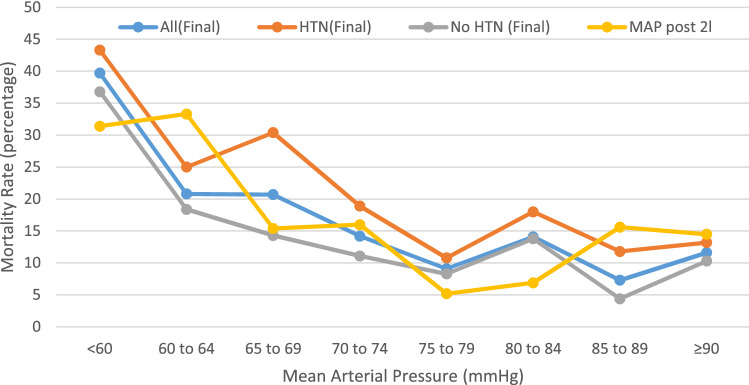
Background: Early treatment is advocated in the management of patients with suspected sepsis in the emergency department (ED). We sought to understand the association between the ED treatments and outcome in patients admitted with suspected sepsis. The treatments studied were: (i) the time to antibiotics, where time zero is the time the patient was booked in which is also the triage time; (ii) the volume of intravenous fluid (IVF); (iii) mean arterial pressure (MAP) after 2000 ml of IVF and (iv) the final MAP in the ED.
Methods: We performed a retrospective analysis of the ED database of patients aged ≥ 18 year who met two SIRS criteria or one red flag sepsis criteria on arrival, received intravenous antibiotics for a suspected infection and admitted between 8th February 2016 and 31st August 2017. The primary outcome measure was all-cause in-hospital mortality. The four treatments stated above were controlled for severity of illness and subject to multivariate logistic regression and Cox proportional-hazard regression to identify independent predictors of mortality.
Results: Of the 2,066 patients studied 272 (13.2%) died in hospital. The median time to antibiotics was 48 (interquartile range 30-82) minutes. The time to antibiotics was an independent predictor of mortality only in those who developed refractory hypotension (RH); antibiotics administered more than 55 mins after arrival was associated with an odds ratio (OR) for mortality of 2.75 [95% confidence interval (CI) 1.22-6.14]. The number-needed-to-treat was 4. IVF > 2000 ml (95% CI > 500- > 2100), except in RH, and a MAP ≤ 66 mmHg after 2000 ml of IVF were also independent predictors of mortality. The OR for mortality of IVF > 2,000 ml in non-RH was 1.80 (95% CI 1.15-2.82); Number-needed-to-harm was 14. The OR for morality for a MAP ≤ 66 mmHg after 2000 ml of IVF was 3.42 (95% CI 2.10-5.57). A final MAP < 75 mmHg in the ED was associated with, but not an independent predictor of mortality. An initial systolic blood pressure of < 100 mmHg has a sensitivity of 63.3% and specificity of 88.4% for the development of RH.
Conclusion: In this study, antibiotics were found to be time-critical in RH. Intravenous fluids > 2000 ml (except in RH) and a MAP ≤ 66 mmHg after 2000 ml of IVF were also independent predictors of mortality.
Keywords: Antibiotics; Blood pressure; Emergency department; Sepsis; Septic shock; Time-to-treatment.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- UK Sepsis Trust. Guidance for professionals. https://sepsistrust.org/wp-content/uploads/2020/08/Sepsis-Acute-12-1.3.pdf Accessed 14 Sep 2020
-
- National Institute of Health and Care Excellence. Sepsis: recognition, diagnosis and early management. https://www.nice.org.uk/guidance/NG51 - PubMed
-
- Szakmany T, Lundin RM, Sharif B, Ellis G, Morgan P. Kopczynska M et al Sepsis prevalence and outcome on the general wards and emergency departments in wales: results of a multi-centre, observational, point-prevalence study. PLoS ONE. 2016;11(12):e0167230. doi: 10.1371/journal.pone.0167230. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
