

Children with refractory epilepsy demonstrate alterations in myocardial strain
- PMID: 33053223
- PMCID: PMC8191539
- DOI: 10.1111/epi.16652
Children with refractory epilepsy demonstrate alterations in myocardial strain
Abstract
Objective: To test whether children with epilepsy have impairments in myocardial mechanics compared to controls without epilepsy.
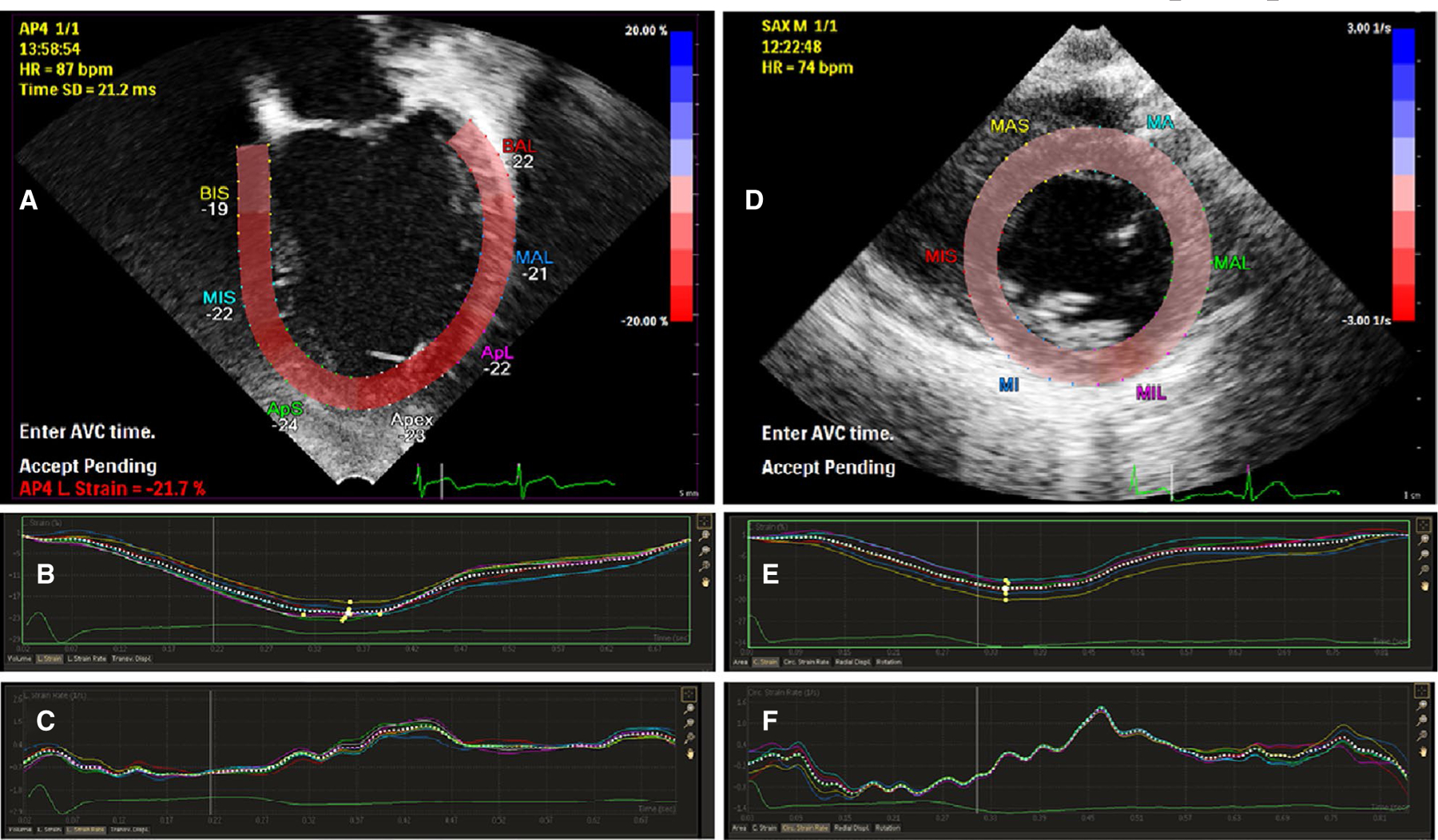
Methods: Children with refractory epilepsy with epilepsy duration of at least 3 years underwent echocardiography including conventional measurements and speckle tracking to assess longitudinal and circumferential strain. Parent-completed surveys, capturing critical aspects of the children's seizure history and cardiac risk factors, complemented retrospective chart reviews, which also included antiepileptic drug history. Normal echocardiograms from controls, matched for age and gender, were obtained from our institutional database and evaluated for strain.
Results: Forty-one patients (median age = 10 years, interquartile range [IQR] = 5-15; 58.5% male) were enrolled. Epilepsy etiology included genetic (n = 26), structural (n = 6), genetic and structural (n = 5), infection (n = 3), and unknown (n = 1). No cardiac structural abnormalities were identified. Both longitudinal and circumferential strain were impaired (P < .03) in patients compared to controls (median [IQR] = 22.7% [21.2-24.2] vs 23.6% [22.2-26.1] and 22.0% [20.3-25.4] vs 24.5% [22.3-27.0], respectively), indicating decreased myocardial deformation/contraction. Shortening fraction was higher in patients (37.6% [35.7-39.7] vs 34.9% [32.5-38.7], P = .009); mitral valve E wave inflow velocity (84.8 cm/s [78.4-92.8] vs 97.2 cm/s [85.9-105.8], P = .005) and tissue Doppler lateral E' wave (13.9 cm/s [12.3-16.1] vs 17.3 cm/s [15.4-18.5], P < .001) were decreased compared to controls. Findings were similar in the pairs with epilepsy patients distinguished by the ability to independently ambulate. There was no difference between patients and controls in ejection fraction. Among the epilepsy patients, there were no associations between cardiac measurements and epilepsy characteristics, including seizure type and frequency and cardiotoxic antiseizure medication exposure after correction for multiple comparisons.
Significance: Children with refractory epilepsy had impaired systolic ventricular strain compared to controls, not correlated with epilepsy history. Further studies are needed to determine the significance of these changes.
Keywords: biomarker; cardiac; refractory epilepsy.
© 2020 International League Against Epilepsy.
Conflict of interest statement
CONFLICT OF INTEREST
None of the authors has any conflict of interest to disclose.
Figures
Comment in
-
Echocardiography in epilepsy: A tool to be explored.Epilepsia. 2021 May;62(5):1285-1286. doi: 10.1111/epi.16879. Epub 2021 Mar 23. Epilepsia. 2021. PMID: 33755989 No abstract available.
-
Response: Let us not miss the forest for the trees. Reply to "Echocardiography in epilepsy: A tool to be explored".Epilepsia. 2021 May;62(5):1287-1288. doi: 10.1111/epi.16881. Epub 2021 Mar 23. Epilepsia. 2021. PMID: 33755999 No abstract available.
References
-
- Devinsky O, Hesdorffer DC, Thurman DJ, Lhatoo S, Richerson G. Sudden unexpected death in epilepsy: epidemiology, mechanisms, and prevention. Lancet Neurol 2016;15:1075–88. - PubMed
-
- Legriel S, Bruneel F, Dalle L, Appere-de-Vecchi C, Georges JL, Abbosh N, et al. Recurrent takotsubo cardiomyopathy triggered by convulsive status epilepticus. Neurocrit Care 2008;9:118–21. - PubMed
-
- Shimizu M, Kagawa A, Takano T, Masai H, Miwa Y. Neurogenic stunned myocardium associated with status epilepticus and postictal catecholamine surge. Intern Med 2008;47:269–73. - PubMed
-
- Stöllberger C, Wegner C, Finsterer J. Seizure-associated takotsubo cardiomyopathy. Epilepsia 2011;52:e160–7. - PubMed
-
- Natelson BH, Suarez RV, Terrence CF, Turizo R. Patients with epilepsy who die suddenly have cardiac disease. Arch Neurol 1998;55:857–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
