

Skin Manifestations in COVID-19: Prevalence and Relationship with Disease Severity
- PMID: 33053817
- PMCID: PMC7599735
- DOI: 10.3390/jcm9103261
Skin Manifestations in COVID-19: Prevalence and Relationship with Disease Severity
Abstract
Background: Data on the clinical patterns and histopathology of SARS-CoV-2 related skin lesions, as well as on their relationship with the severity of COVID-19 are limited.
Methods and materials: Retrospective analysis of a prospectively collected cohort of patients with SARS-CoV-2 infection in a teaching hospital in Barcelona, Spain, from 1 April to 1 May 2020. Clinical, microbiological and therapeutic characteristics, clinicopathological patterns of skin lesions, and direct immunofluorescence and immunohistochemical findings in skin biopsies were analyzed.
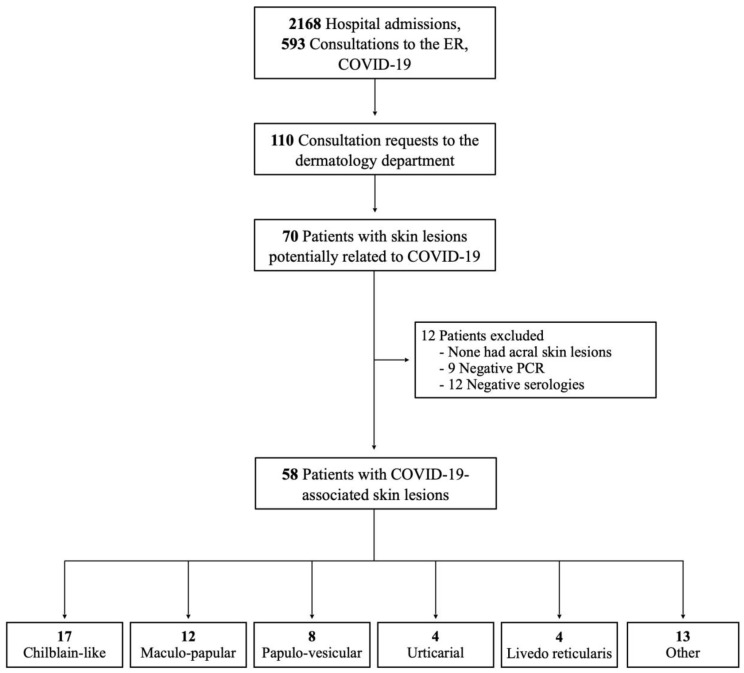
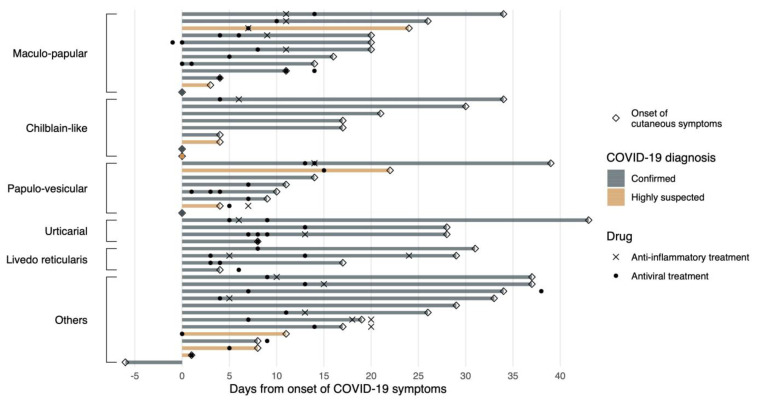
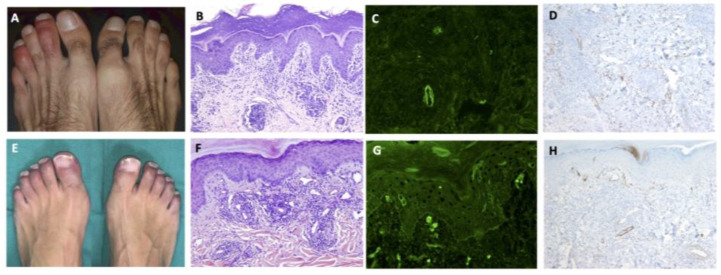
Results: Fifty-eight out of the 2761 patients (2.1%) either consulting to the emergency room or admitted to the hospital for COVID-19 suspicion during the study period presented COVID-19 related skin lesions. Cutaneous lesions could be categorized into six patterns represented by the acronym "GROUCH": Generalized maculo-papular (20.7%), Grover's disease and other papulo-vesicular eruptions (13.8%), livedo Reticularis (6.9%), Other eruptions (22.4%), Urticarial (6.9%), and CHilblain-like (29.3%). Skin biopsies were performed in 72.4%, including direct immunofluorescence in 71.4% and immunohistochemistry in 28.6%. Patients with chilblain-like lesions exhibited a characteristic histology and were significantly younger and presented lower rates of systemic symptoms, radiological lung infiltrates and analytical abnormalities, and hospital and ICU admission compared to the rest of patients.
Conclusion: Cutaneous lesions in patients with COVID-19 appear to be relatively rare and varied. Patients with chilblain-like lesions have a characteristic clinicopathological pattern and a less severe presentation of COVID-19.
Keywords: COVID-19; chilblain; coronavirus; histopathology; pandemic; skin lesions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- COVID-19 Map. [(accessed on 3 May 2020)]; Available online: https://coronavirus.jhu.edu/map.html.
-
- Bikdeli B., Madhavan M.V., Jimenez D., Chuich T., Dreyfus I., Driggin E., Nigoghossian C.D., Ageno W., Madjid M., Guo Y., et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up. J. Am. Coll. Cardiol. 2020;75:2950–2973. doi: 10.1016/j.jacc.2020.04.031. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
