

Chronic lymphocytic leukemia: from molecular pathogenesis to novel therapeutic strategies
- PMID: 33054046
- PMCID: PMC7556519
- DOI: 10.3324/haematol.2019.236000
Chronic lymphocytic leukemia: from molecular pathogenesis to novel therapeutic strategies
Abstract
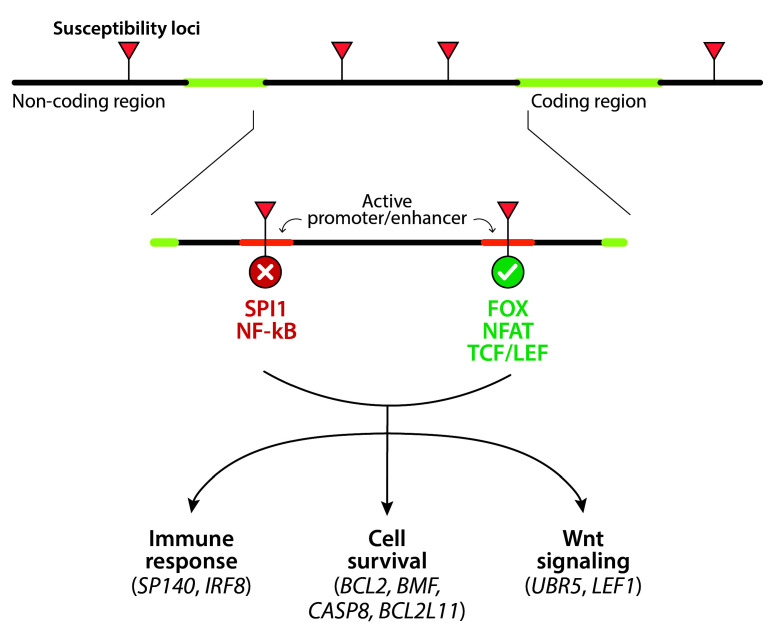
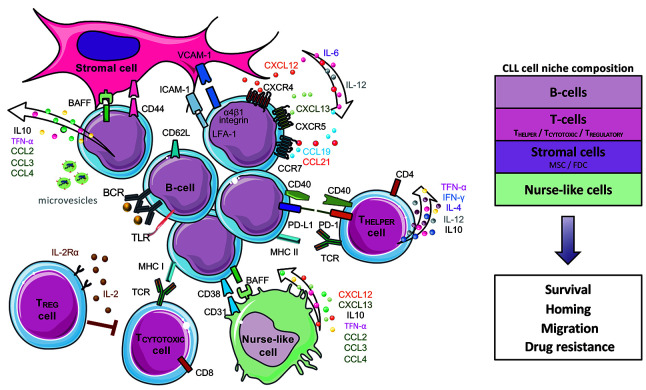
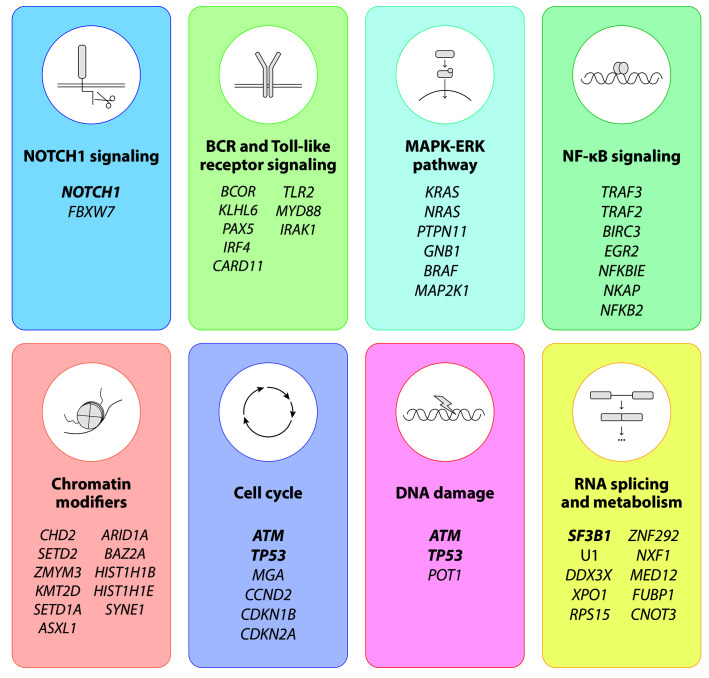
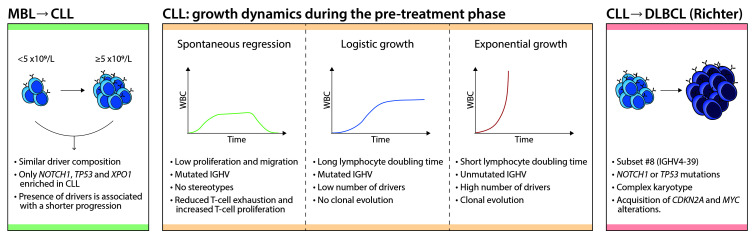
Chronic lymphocytic leukemia is a well-defined lymphoid neoplasm with very heterogeneous biological and clinical behavior. The last decade has been remarkably fruitful in novel findings elucidating multiple aspects of the pathogenesis of the disease including mechanisms of genetic susceptibility, insights into the relevance of immunogenetic factors driving the disease, profiling of genomic alterations, epigenetic subtypes, global epigenomic tumor cell reprogramming, modulation of tumor cell and microenvironment interactions, and dynamics of clonal evolution from early steps in monoclonal B cell lymphocytosis to progression and transformation into diffuse large B-cell lymphoma. All this knowledge has offered new perspectives that are being exploited therapeutically with novel target agents and management strategies. In this review we provide an overview of these novel advances and highlight questions and perspectives that need further progress to translate into the clinics the biological knowledge and improve the outcome of the patients.
Figures
References
-
- Campo E, Ghia P, Montserrat E, Müller-Hermelink HK, Stein H, Swerdlow SH. Chronic lymphocytic leukaemia/small lymphocytic lymphoma. WHO Classification of Tumours of Haemato - poietic and Lymphoid Tissues. Rev 4th Ed. Lyon: WHO Press; 2017:216-221.
-
- Howlader N, Noone A, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2016, National Cancer Institute. Bethesda, MD, USA.
-
- Puente XS, Beà S, Valdés-Mas R, et al. Noncoding recurrent mutations in chronic lymphocytic leukaemia. Nature. 2015;526 (7574):519-524. - PubMed
-
- Kulis M, Heath S, Bibikova M, et al. Epigenomic analysis detects widespread gene-body DNA hypomethylation in chronic lymphocytic leukemia. Nat Genet. 2012;44(11):1236-1242. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
