

doi: 10.3324/haematol.2019.230276.
Safety and efficacy of brentuximab vedotin as a treatment for lymphoproliferative disorders in primary immunodeficiencies
Affiliations
- PMID: 33054064
- PMCID: PMC7556515
- DOI: 10.3324/haematol.2019.230276
Item in Clipboard
Safety and efficacy of brentuximab vedotin as a treatment for lymphoproliferative disorders in primary immunodeficiencies
Haematologica.
.
No abstract available
Figures
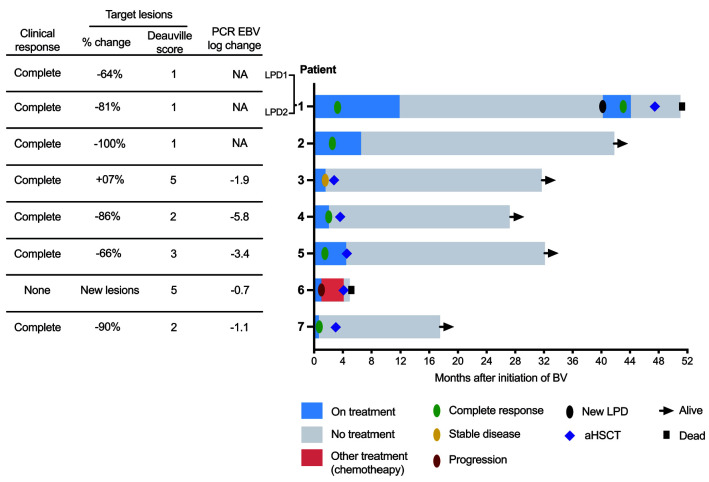
Efficacy of brentuximab vedotin. (Right) Swimmer plot of individual outcome. On the left, summary of clinical response, radiological response of target lesions according to Response Evaluation Criteria in Lymphoma criteria (% change in sum of diameters of target lesions) and metabolic uptake on [18F]2-fluoro- 2-deoxy-D-glucose positron emission tomography-computed tomography and polymerase chain reaction (PCR) Epstein Barr virus (EBV) log change for EBV-related B-cell lymphoproliferative disorder (LPD). In three cases, brentuximab vedotin (BV) was started while the LPD was in a partial response after two courses of COP (cyclophosphamide, vincristine and prednisone) for the LPD1 of P1, one injection of rituximab (375mg/m) and ten days of steroids for P2, and five injections of rituximab (375 mg/m) for P4. In two cases (P3 and P7), the LPD was refractory to rituximab. P1 presented a second LPD, or an immunogenetically evolved relapse, which was not associated with a loss of CD30 expression. The median time to an objective response was 2.6 months (range, 0.56-3.91). However, a clinical improvement was apparent in the first weeks after treatment. aHSCT: allogeneic hematopoietic stem cell transplantation.
References
-
- Pinkerton CR, Hann I, Weston CL, et al. Immunodeficiency-related lymphoproliferative disorders: prospective data from the United Kingdom Children’s Cancer Study Group Registry. Br J Haematol. 2002;118(2):456-461. - PubMed
-
- Cohen JM, Sebire NJ, Harvey J, et al. Successful treatment of lymphoproliferative disease complicating primary immunodeficiency/immunodysregulatory disorders with reducedintensity allogeneic stem-cell transplantation. Blood. 2007; 110(6):2209-2214. - PubMed
-
- Eichenauer DA, Plütschow A, Kreissl S, et al. Incorporation of brentuximab vedotin into first-line treatment of advanced classical Hodgkin’s lymphoma: final analysis of a phase 2 randomised trial by the German Hodgkin Study Group. Lancet Oncol. 2017;18(12):1680-1687. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
