

Does distance from a clinic and poverty impact visit adherence for noncommunicable diseases? A retrospective cohort study using electronic medical records in rural Haiti
- PMID: 33054756
- PMCID: PMC7556963
- DOI: 10.1186/s12889-020-09652-y
Does distance from a clinic and poverty impact visit adherence for noncommunicable diseases? A retrospective cohort study using electronic medical records in rural Haiti
Abstract
Background: Adherence to regular outpatient visits is vital to managing noncommunicable diseases (NCDs), a growing burden in low and middle-income countries. We characterized visit adherence among patients with NCDs in rural Haiti, hypothesizing higher poverty and distance from the clinic were associated with lower adherence.
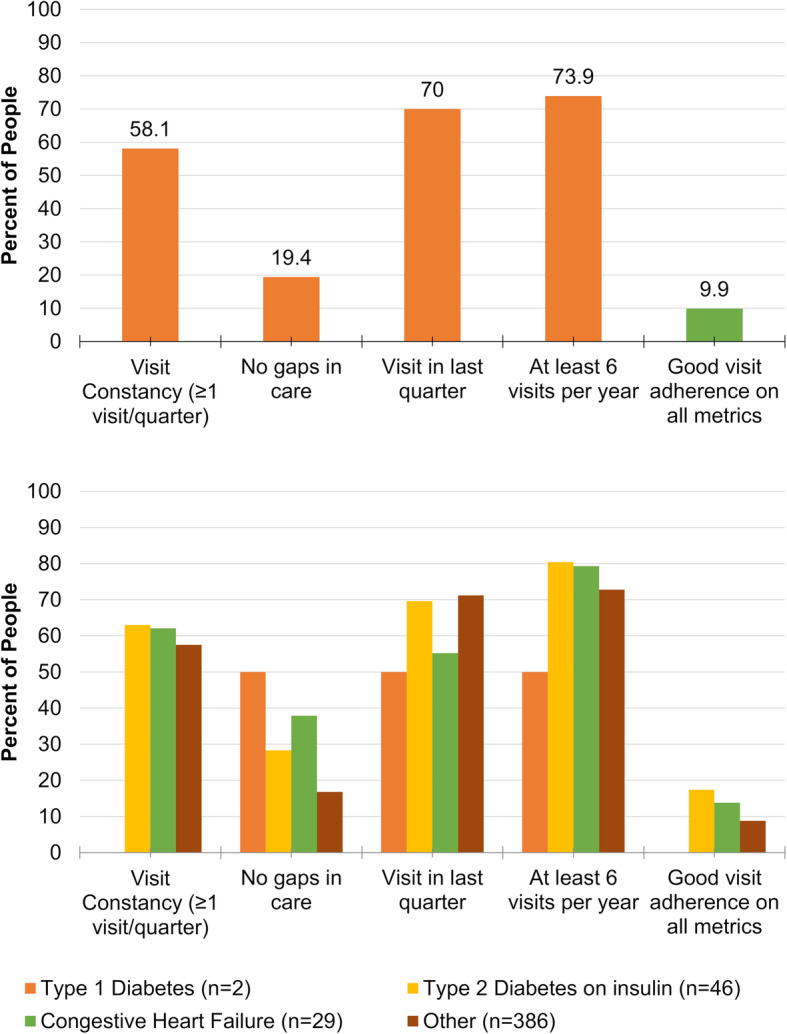
Methods: We analyzed electronic medical records from a cohort of adults in an NCD clinic in Mirebalais, Haiti (April 2013 to June 2016). Visit adherence was: 1) visit constancy (≥1 visit every 3 months), 2) no gaps in care (> 60 days between visits), 3) ≥1 visit in the last quarter, and 4) ≥6 visits per year. We incorporated an adapted measure of intensity of multidimensional poverty. We calculated distance from clinic as Euclidean distance or self-reported transit time. We used multivariable logistic regressions to assess the association between poverty, distance, and visit adherence.
Results: We included 463 adult patients, mean age 57.8 years (SE 2.2), and 72.4% women. Over half of patients had at least one visit per quarter (58.1%), but a minority (19.6%) had no gaps between visits. Seventy percent of patients had a visit in the last quarter, and 73.9% made at least 6 visits per year. Only 9.9% of patients met all adherence criteria. In regression models, poverty was not associated with any adherence measures, and distance was only associated with visit in the last quarter (OR 0.87, 95% CI [0.78 to 0.98], p = 0.03) after adjusting for age, sex, and hardship financing.
Conclusions: Visit adherence was low in this sample of adult patients presenting to a NCD Clinic in Haiti. Multidimensional poverty and distance from clinic were not associated with visit adherence measures among patients seen in the clinic, except for visit in the last quarter. Future research should focus on identifying and addressing barriers to visit adherence.
Keywords: Global health; Haiti; Noncommunicable disease; Retention in care; Visit adherence.
Conflict of interest statement
EJB reports grants from NHLBI, R01HL128914; 2R01 HL092577; 1R01 HL141434 01A1; 2U54HL120163; 1R01AG066010; and a grant from American Heart Association, 18SFRN34110082 during the conduct of the study. The remaining authors report no conflicts of interest related to the study.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
