

Effectiveness of pelvic floor muscle training with and without electromyographic biofeedback for urinary incontinence in women: multicentre randomised controlled trial
- PMID: 33055247
- PMCID: PMC7555069
- DOI: 10.1136/bmj.m3719
Effectiveness of pelvic floor muscle training with and without electromyographic biofeedback for urinary incontinence in women: multicentre randomised controlled trial
Abstract
Objective: To assess the effectiveness of pelvic floor muscle training (PFMT) plus electromyographic biofeedback or PFMT alone for stress or mixed urinary incontinence in women.
Design: Parallel group randomised controlled trial.
Setting: 23 community and secondary care centres providing continence care in Scotland and England.
Participants: 600 women aged 18 and older, newly presenting with stress or mixed urinary incontinence between February 2014 and July 2016: 300 were randomised to PFMT plus electromyographic biofeedback and 300 to PFMT alone.
Interventions: Participants in both groups were offered six appointments with a continence therapist over 16 weeks. Participants in the biofeedback PFMT group received supervised PFMT and a home PFMT programme, incorporating electromyographic biofeedback during clinic appointments and at home. The PFMT group received supervised PFMT and a home PFMT programme. PFMT programmes were progressed over the appointments.
Main outcome measures: The primary outcome was self-reported severity of urinary incontinence (International Consultation on Incontinence Questionnaire-urinary incontinence short form (ICIQ-UI SF), range 0 to 21, higher scores indicating greater severity) at 24 months. Secondary outcomes were cure or improvement, other pelvic floor symptoms, condition specific quality of life, women's perception of improvement, pelvic floor muscle function, uptake of other urinary incontinence treatment, PFMT self-efficacy, adherence, intervention costs, and quality adjusted life years.
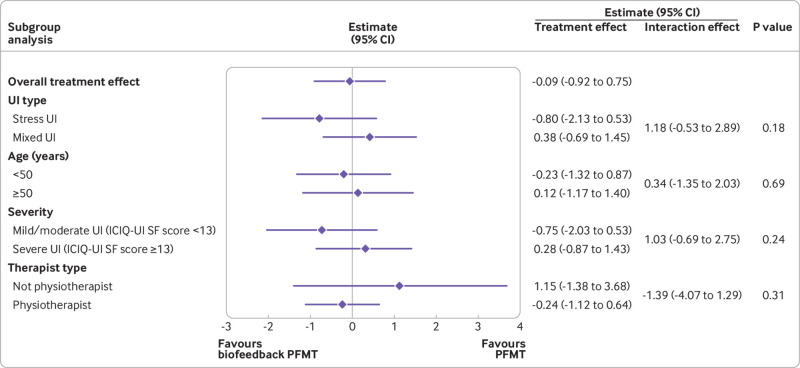
Results: Mean ICIQ-UI SF scores at 24 months were 8.2 (SD 5.1, n=225) in the biofeedback PFMT group and 8.5 (SD 4.9, n=235) in the PFMT group (mean difference -0.09, 95% confidence interval -0.92 to 0.75, P=0.84). Biofeedback PFMT had similar costs (mean difference £121 ($154; €133), -£409 to £651, P=0.64) and quality adjusted life years (-0.04, -0.12 to 0.04, P=0.28) to PFMT. 48 participants reported an adverse event: for 23 this was related or possibly related to the interventions.
Conclusions: At 24 months no evidence was found of any important difference in severity of urinary incontinence between PFMT plus electromyographic biofeedback and PFMT alone groups. Routine use of electromyographic biofeedback with PFMT should not be recommended. Other ways of maximising the effects of PFMT should be investigated.
Trial registration: ISRCTN57756448.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form. All authors declare grant funding for the trial from National Institute for Health Research (NIHR), Health Technology Assessment programme. In addition, outside the submitted work WA reports: personal fees from UCB Pharma, Pfizer, Bard, Boston Scientific, Neomedic, Johnson and Johnson, SEP Pharma/Contura, NHS Ayrshire and Arran, London Medical Education Academy, Central Legal Office NHS Scotland, Oaklaw Consultancy, various law firms acting on behalf of mesh manufacturers, patient claimants, and defendant clinicians; grants from Olympus, NIHR, University of Stirling, University of Aberdeen; grants and non-financial support from Astellas Pharmaceuticals; personal fees and non-financial support from Chief Scientist Office, NHS Research Scotland, and NHS Ayrshire and Arran. KG reports personal fees and non-financial support from Contura, outside the submitted work. MAF reports outside the submitted work: being a speaker, consultant and/or surgical trainer for a number of industrial companies (Astellas, Ethicon, Bard, Pfizer, AMS, Coloplast, and others); receiving travel expenses and received personal honorariums and sponsorship towards attending scientific conferences and educational meetings; research grant from Coloplast; sponsorship for trainees attending or presenting at pharmaceutical sponsored educational/ leadership workshops and scientific conferences; being previous chairman of the Scottish Pelvic Floor Network, which received sponsorship by various industrial companies. JN reports outside the submitted work membership of the following NIHR boards: Commissioning Priority Review Decision-making committee (2015); Health Technology Assessment (HTA) Commissioning Board (2010-2016); HTA Commissioning Sub-Board (Expression of Interest) (2014); HTA Funding Boards Policy Group (2016-2019); HTA General Board (2016-2019); HTA Post-Board funding teleconference (2016-2019); NIHR Clinical Trials Unit Standing Advisory Committee (2018-present); NIHR HTA and Efficacy and Mechanism Evaluation Editorial Board (2014-2019); Pre-exposure Prophylaxis Impact Review Panel (2017).
Figures

Comment in
-
Voiding Function and Dyfunction, Bladder Physiology and Pharmacology, and Female Urology.J Urol. 2021 May;205(5):1519-1524. doi: 10.1097/JU.0000000000001675. Epub 2021 Feb 24. J Urol. 2021. PMID: 33625243 No abstract available.
References
-
- Abrams P, Cardozo L, Fall M, et al. Standardisation Sub-committee of the International Continence Society The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002;21:167-78. 10.1002/nau.10052 - DOI - PubMed
-
- National, Guideline Alliance UK. Urinary incontinence and pelvic organ prolapse in women: management. 2019. - PubMed
-
- Bo K, Frawley HC, Haylen BT, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Int Urogynecol J 2017;28:191-213. 10.1007/s00192-016-3123-4 - DOI - PubMed
-
- Herderschee R, Hay-Smith EJ, Herbison GP, Roovers JP, Heineman MJ. Feedback or biofeedback to augment pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst Rev 2011;(7):CD009252. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical