

Differentiating Staphylococcus infection-associated glomerulonephritis and primary IgA nephropathy: a mass spectrometry-based exploratory study
- PMID: 33057112
- PMCID: PMC7560901
- DOI: 10.1038/s41598-020-73847-x
Differentiating Staphylococcus infection-associated glomerulonephritis and primary IgA nephropathy: a mass spectrometry-based exploratory study
Abstract
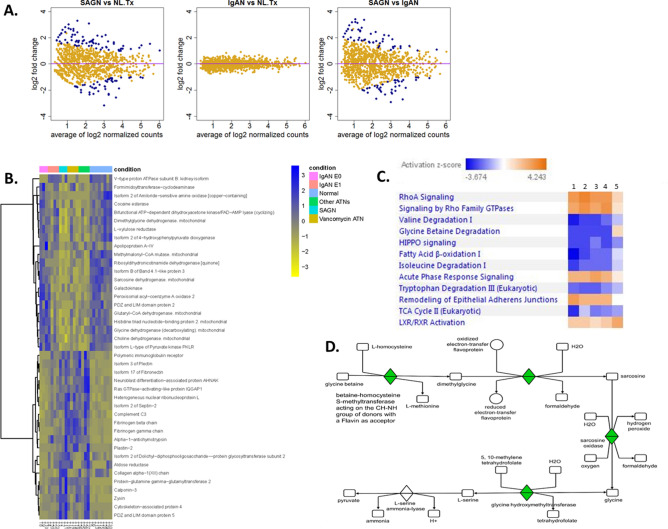
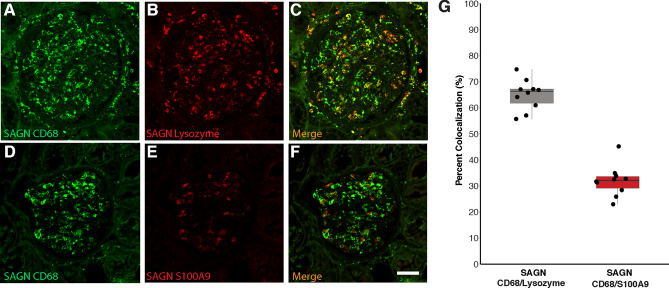
Staphylococcus infection-associated glomerulonephritis (SAGN) and primary IgA nephropathy (IgAN) are separate disease entities requiring different treatment approaches. However, overlapping histologic features may cause a diagnostic dilemma. An exploratory proteomic study to identify potential distinguishing biomarkers was performed on formalin fixed paraffin embedded kidney biopsy tissue, using mass spectrometry (HPLC-MS/MS) (n = 27) and immunohistochemistry (IHC) (n = 64), on four main diagnostic groups-SAGN, primary IgAN, acute tubular necrosis (ATN) and normal kidney (baseline transplant biopsies). Spectral counts modeled as a negative binomial distribution were used for statistical comparisons and in silico pathway analysis. Analysis of variance techniques were used to compare groups and the ROC curve to evaluate classification algorithms. The glomerular proteomes of SAGN and IgAN showed remarkable similarities, except for significantly higher levels of monocyte/macrophage proteins in SAGN-mainly lysozyme and S100A9. This finding was confirmed by IHC. In contrast, the tubulointerstitial proteomes were markedly different in IgAN and SAGN, with a lower abundance of metabolic pathway proteins and a higher abundance of extracellular matrix proteins in SAGN. The stress protein transglutaminase-2 (TGM2) was also significantly higher in SAGN. IHC of differentially-expressed glomerular and tubulointerstitial proteins can be used to help discriminate between SAGN and IgAN in ambiguous cases.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Satoskar AA, Nadasdy T, Silva FG. Acute post-infectious glomerulonephritis and Glomerulonephritis caused by persistent bacterial infection. Chapter 10. In: Jennette JC, Olson JL, D’Agati VD, Silva F, editors. Heptinstall’s Pathology of the Kidney. 7. Philadelphia: LWW; 2014. pp. 367–436.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
