

Magnitude, demographics and dynamics of the effect of the first wave of the COVID-19 pandemic on all-cause mortality in 21 industrialized countries
- PMID: 33057181
- PMCID: PMC7615092
- DOI: 10.1038/s41591-020-1112-0
Magnitude, demographics and dynamics of the effect of the first wave of the COVID-19 pandemic on all-cause mortality in 21 industrialized countries
Erratum in
-
Author Correction: Magnitude, demographics and dynamics of the effect of the first wave of the COVID-19 pandemic on all-cause mortality in 21 industrialized countries.Nat Med. 2021 Mar;27(3):562. doi: 10.1038/s41591-021-01254-4. Nat Med. 2021. PMID: 33531711 Free PMC article. No abstract available.
Abstract
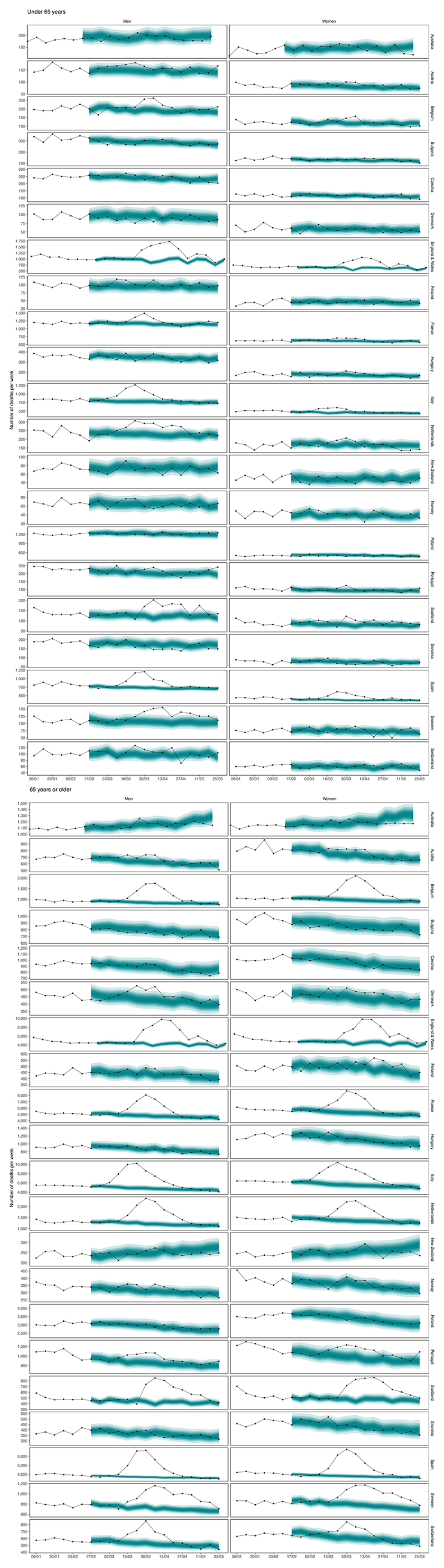
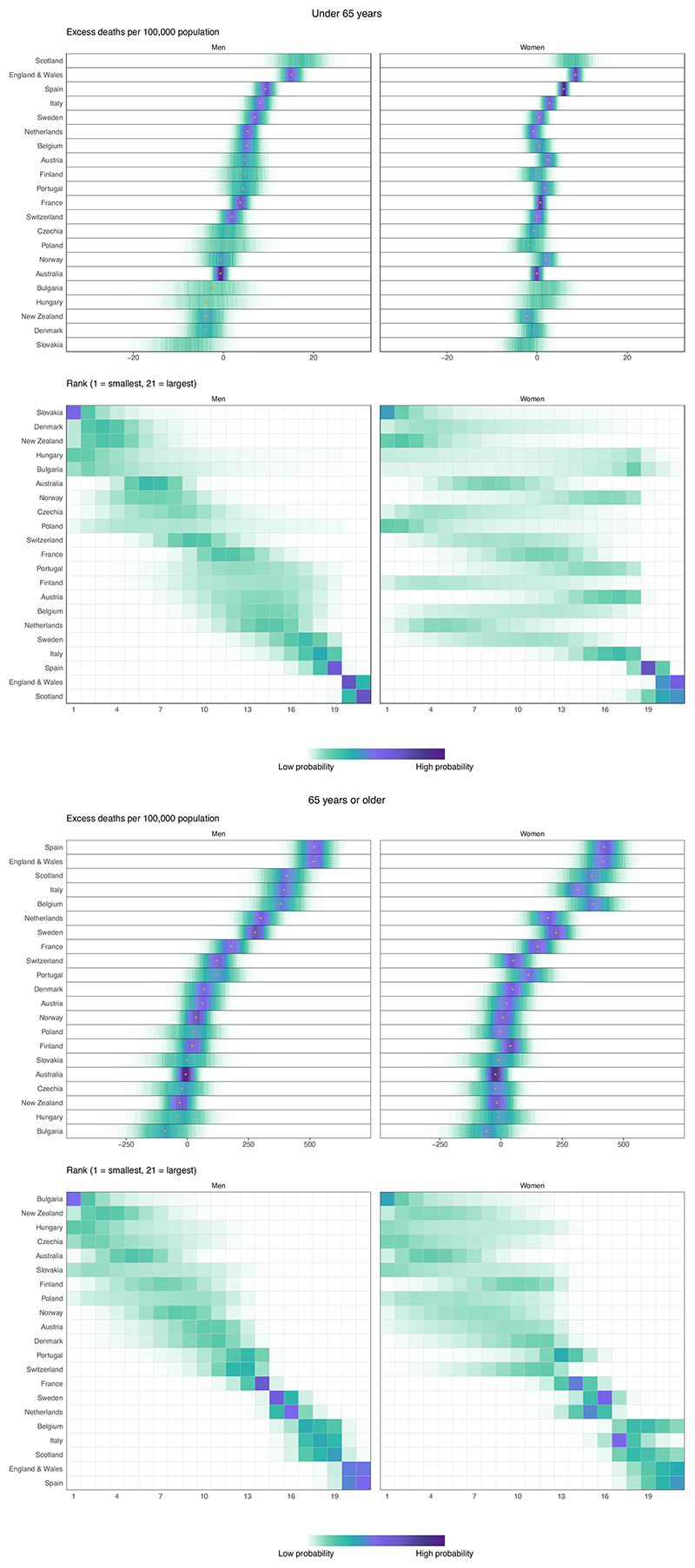
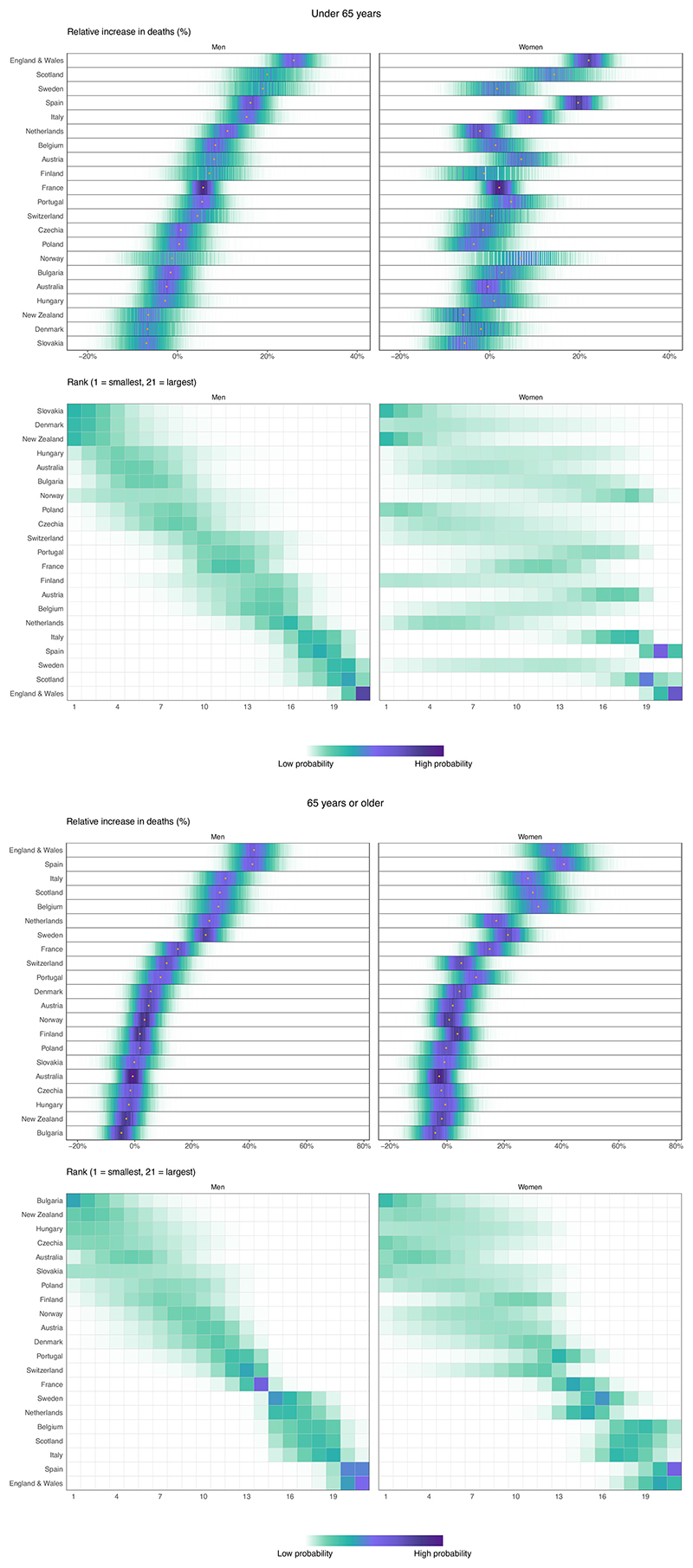
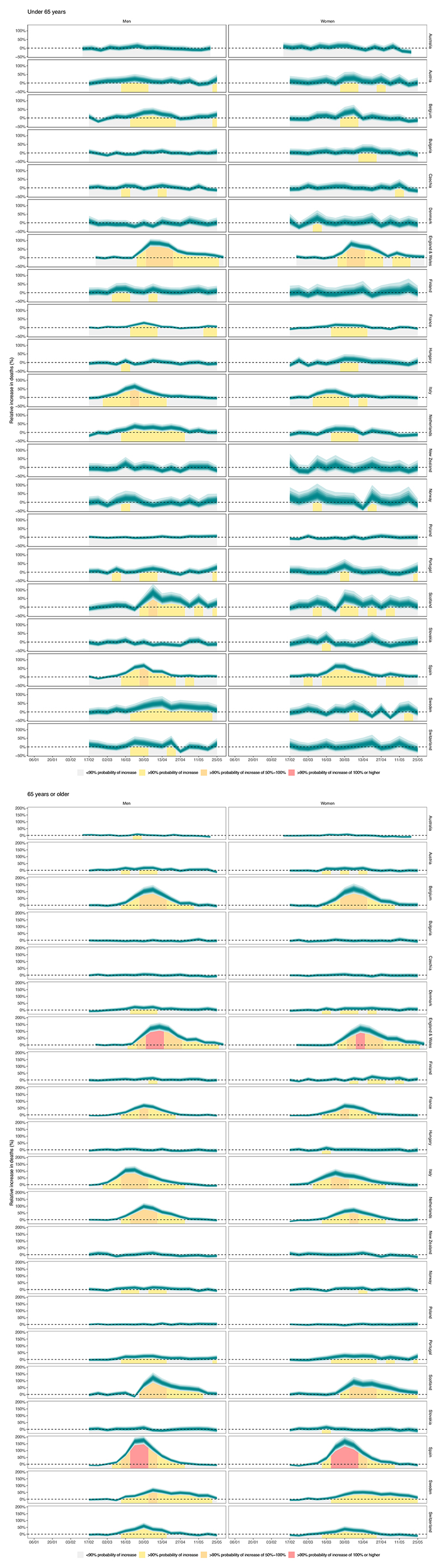
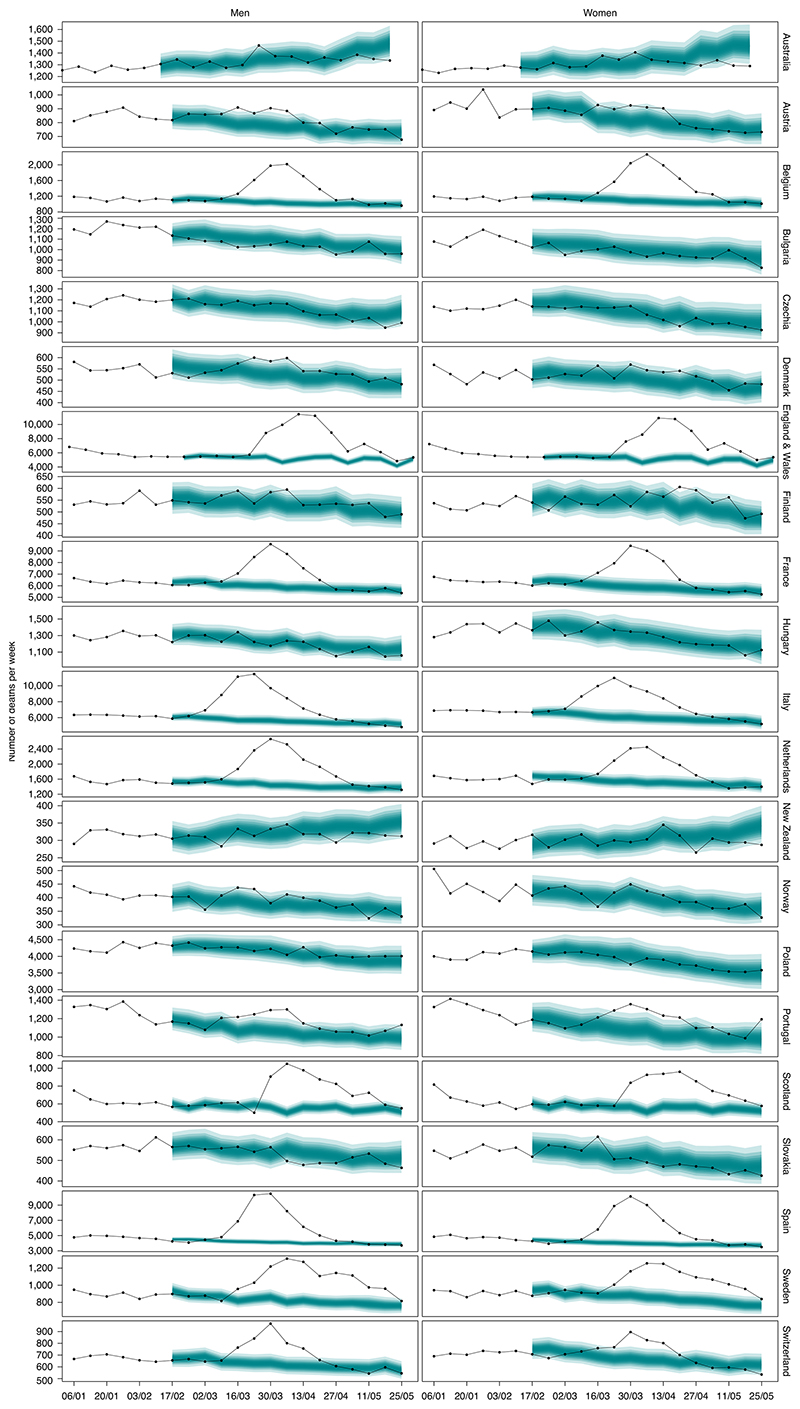
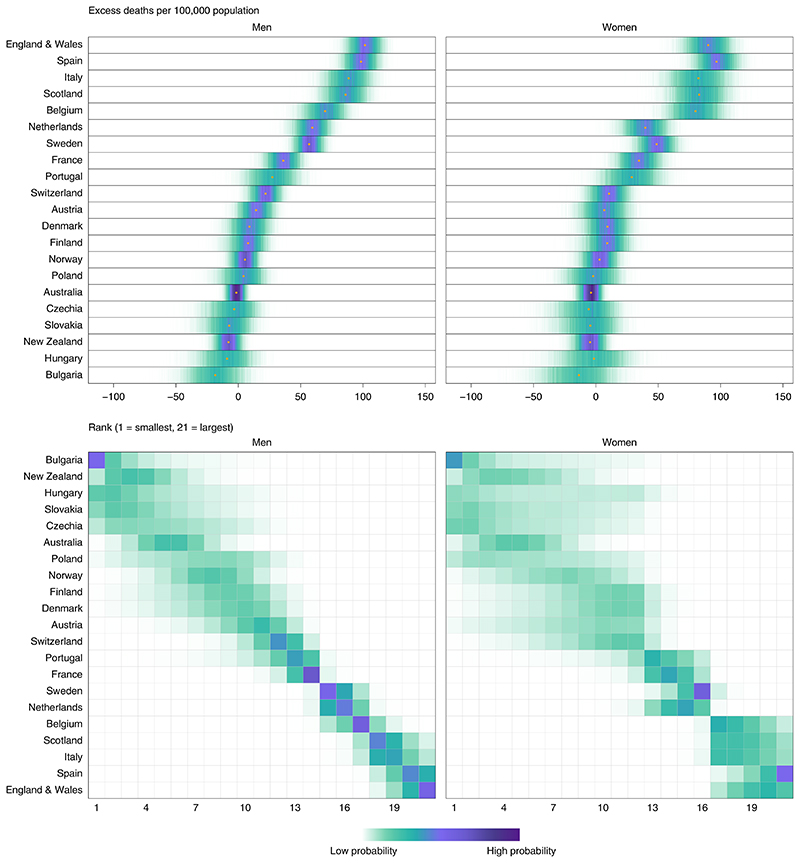
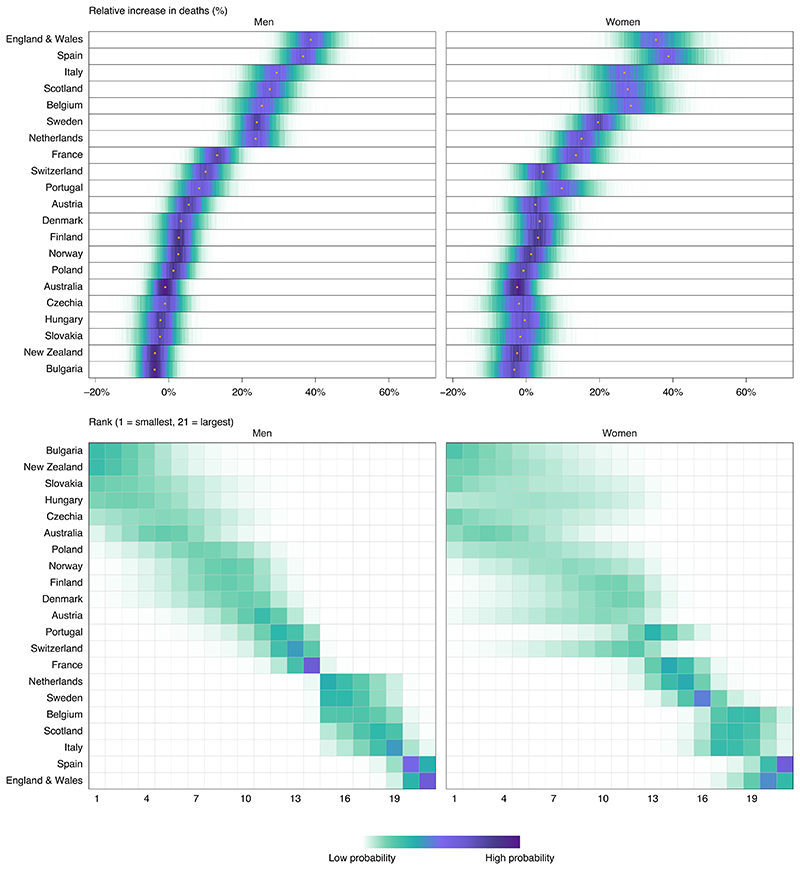
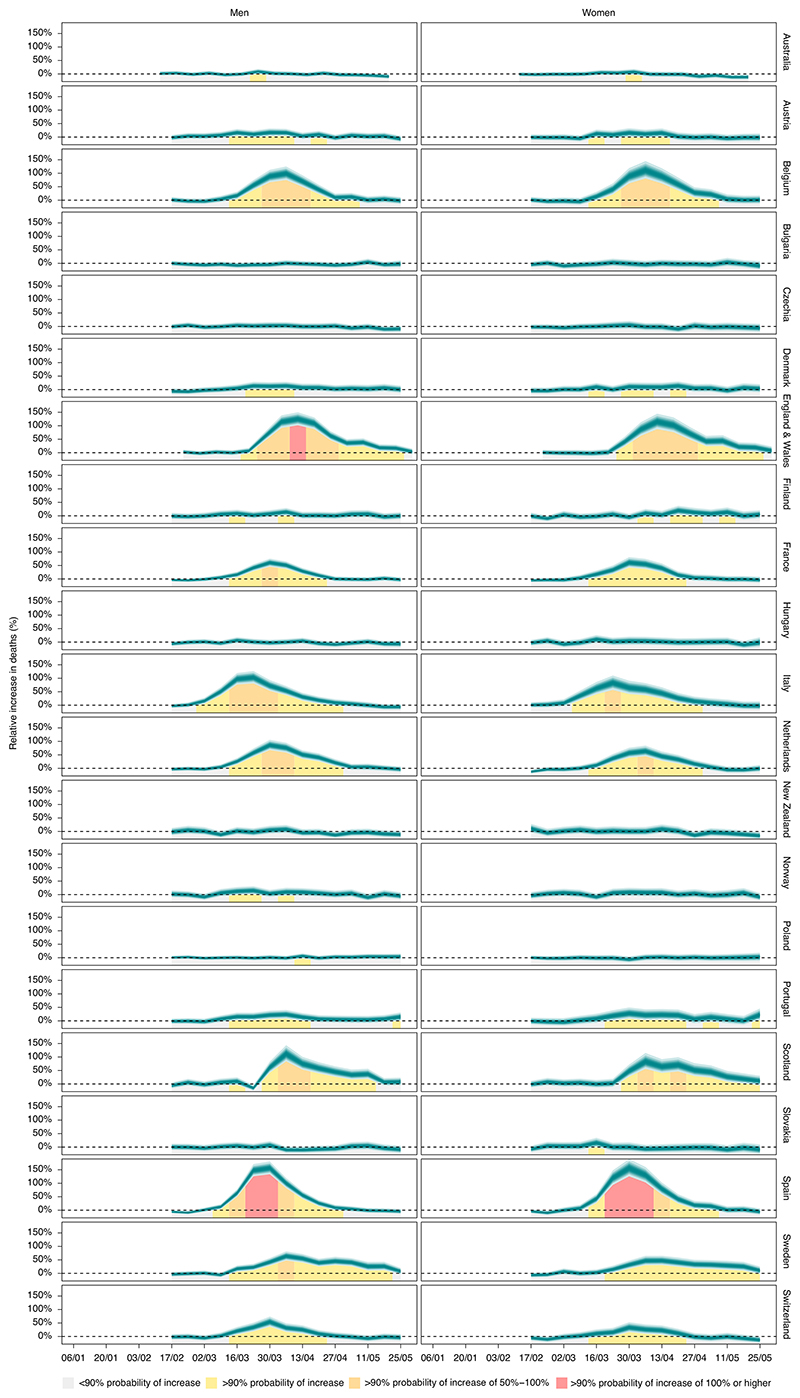
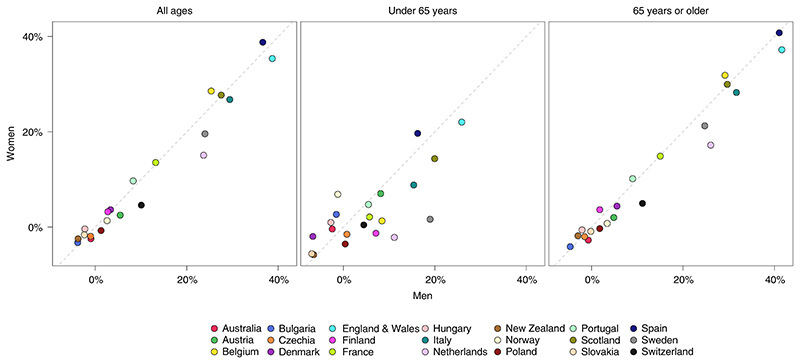
The Coronavirus Disease 2019 (COVID-19) pandemic has changed many social, economic, environmental and healthcare determinants of health. We applied an ensemble of 16 Bayesian models to vital statistics data to estimate the all-cause mortality effect of the pandemic for 21 industrialized countries. From mid-February through May 2020, 206,000 (95% credible interval, 178,100-231,000) more people died in these countries than would have had the pandemic not occurred. The number of excess deaths, excess deaths per 100,000 people and relative increase in deaths were similar between men and women in most countries. England and Wales and Spain experienced the largest effect: ~100 excess deaths per 100,000 people, equivalent to a 37% (30-44%) relative increase in England and Wales and 38% (31-45%) in Spain. Bulgaria, New Zealand, Slovakia, Australia, Czechia, Hungary, Poland, Norway, Denmark and Finland experienced mortality changes that ranged from possible small declines to increases of 5% or less in either sex. The heterogeneous mortality effects of the COVID-19 pandemic reflect differences in how well countries have managed the pandemic and the resilience and preparedness of the health and social care system.
Conflict of interest statement
M.E. reports a charitable grant from the AstraZeneca Young Health Programme and personal fees from Prudential, outside the submitted work. J.P.-S. is vice-chair of the Royal Society for Public Health and reports personal fees from Novo Nordisk A/S and Lane, Clark & Peacock, outside of the submitted work.
Figures
References
-
- Merrick R. Coronavirus: Boris Johnson’s claim it is ‘too early’ to draw global death toll comparisons mocked by Keir Starmer. The Independent. 2020. https://www.independent.co.uk/news/uk/politics/coronavirus-daily-briefin... .
-
- World Health Organization. Global Health Estimates: Deaths by Cause, Age, Sex and Country, 2000-2016. World Health Organization; 2018.
-
- Fuller T, Baker M. Coronavirus death in California came weeks before first known U.S. death. The New York Times. 2020 https://www.nytimes.com/2020/04/22/us/coronavirus-first-united-states-de... .
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
